
Research Article | DOI: https://doi.org/IJCRI-RA-25-021
Trends In Apolipoprotein and Troponin Levels Among Owerri Residents with Diabetes
Abstract
A cross-sectional study was carried out to determine the levels of apolipoproteins and troponins in individuals with diabetes who were attending the Specialist Hospital Owerri. The study participants included 100 individuals with diabetes and 100 individuals in the control group, all between the ages of 40 and 70. The blood samples were allowed to coagulate, centrifuged, and the serum was used to determine the levels of Troponins 1 and T and Apolipoproteins A-1 and B. The data was analyzed using the statistical program for social sciences, version 21, Windows 9, and the results were expressed as mean ± standard deviation and student t-test. In individuals with diabetes, the ratio of Apolipoproteins B/Apolipoproteins A-1, Troponin 1, Troponin T, and Apolipoprotein B was significantly greater. In relation to sex, male individuals with diabetes exhibited significantly greater Troponin T levels than female individuals with diabetes. Patients with obesity, myocardial infarction, coronary heart disease, artherosclerotic disease, dyslipidemia, vascular hypertrophy, and other complications related to hypertension may benefit from routine laboratory testing where apolipoproteins can be used to predict, manage, and assess the risk of the disease and ultimately improve treatment outcomes.
Introduction:
Diabetes mellitus is a long-term metabolic disease marked by elevated blood sugar levels brought on by deficiencies in either insulin secretion, insulin action, or both. Diabetes is becoming more and more common worldwide, which has serious public health implications, especially in developing nations like Nigeria. [1] Diabetes is becoming more common in Nigeria, according to recent studies, especially in cities like Owerri. Dietary changes, urbanization, and sedentary lifestyles have all contributed to this increase. According to reports, the incidence of diabetes in southeast Nigeria is between 4.6% and 10%, with urban dwellers being more likely to have the disease than rural ones. A number of variables, including the high incidence of overweight and obesity brought on by poor diets and sedentary lifestyles, are contributing to the rising diabetes burden among Owerri citizens. A family history of diabetes raises the risk of getting the condition. Diabetes is frequently linked to high blood pressure. The four types of diabetes mellitus are type-1, type-2, gestational diabetes mellitus, and other specific types of diabetes. Type-1 and type-2 diabetes mellitus are the most common forms of diabetes mellitus.2 According to the International Diabetes Federation (IDF) report, type-2 diabetes became the leading type among all cases of diabetes mellitus, contributing to 90% to 95% of cases in developed countries and may exceed this percentage in developing countries due to urbanization and westernization. Type-1 diabetes mellitus is a chronic metabolic disease marked by elevated blood glucose levels brought on by insulin resistance or insulin deficiency.[2]
The following recent trends demonstrate the growing use of biochemical markers for diabetes diagnosis and treatment: FBG, or fasting blood glucose, is frequently used for preliminary diagnosis.
Information on long-term glycemic control is provided by glycated hemoglobin (HbA1c). Lipid Profiles: Patients with diabetes frequently exhibit dyslipidemia [3].
In fact, apolipoproteins and troponins are receiving more attention for evaluating cardiovascular risk in diabetics. Comprehensive public health initiatives are urgently needed, as evidenced by the escalating trends in diabetes among Owerri inhabitants. Reducing the diabetes epidemic requires early detection, lifestyle changes, and effective management.
Heart troponins are a very sensitive and specific biomarker of myocardial injury, but their function in the present diagnosis of cardiovascular diseases is unappreciated [4].
The contraction of both cardiac and skeletal muscle depends on a class of three regulatory proteins known as troponin, which includes Troponin C, I, and T. When it is connected to the protein tropomyosin, it forms the troponin-tropomyosin system, which is found in the actin filament groove of muscle tissue. When the muscle is relaxed, tropomyosin stops the myosin crossbridge from connecting to the muscle, preventing contraction. However, calcium channels in the sarcoplasmic membrane open, allowing calcium to enter the sarcoplasm when an action potential causes the muscle to contract. Following that, a portion of this calcium binds to troponin, altering its structure and exposing the actin filaments' myosin binding sites, also referred to as active sites. Myosin's binding to actin causes muscle contraction and the formation of crossbridges [5].
As a diagnostic and prognostic indicator, it can be used to treat myocardial infarction, acute coronary syndrome, and stroke. The sarcoplasm reticulum's calcium channels open in response to nerve impulses, letting calcium ions enter the cytoplasm and connect to cardiac troponin C. Conversely, cardiac troponin T (CT-T) promotes the attachment of the troponin-tropomyosin system to thin filament. It also contributes to the conformational changes of the system that, once troponin C binds to calcium ions, cause myosin head binding regions to open during action. The last two proteins interact to form transverse actimyosin bridges, which mediate the contraction of striated muscles.
Cardiac troponin I (CT-I) inhibits the synthesis of actimyosin bridges and is dormant during muscular relaxation. Mutations in the genes encoding cardiac troponins result in disorders of contractile cardiac myocytes. A number of heart failure symptoms might present clinically as contraction-relaxation [6]. Ischemia necrosis causes cardiac myocytes to release the proteins CT-T and CT-I into the bloodstream, which can be used to identify myocardial infarction. Dyslipidemia and hypertension are two recognized modifiable risk factors for cardiovascular disease that frequently co-occur. These are metabolic syndrome components that may share a common cause. Conversely, dyslipidemia is characterized by elevated levels of triglycerides, apolipoprotein B (ApoB), and tiny low-density lipoprotein (LDL) particles and decreased levels of apolipoprotein A and high-density lipoprotein (HDL) cholesterol [7].
Apolipoprotein, a protein component of plasma lipoprotein, is responsible for carrying lipids, or fat molecules, including cholesterol, to every cell in every tissue in the body. The amount of plasma Apolipoprotein B (ApoB) can be used to directly measure the total amount of circulatory anterogenic particles, such as LDL, IDL, and VLDL cholesterol and lipoprotein (a). Several studies have shown that the concentration of Apo B is a more accurate indicator of the risk of cardiovascular disease and a person's susceptibility to lipid-lowering medications than LDL cholesterol, and that there is a significant correlation between plasma ApoB levels and hypertension[8].
Apolipoprotein A1, the main protein that constitutes HDL particles in plasma, aids in the outflow of fat molecules by absorbing lipids from within cells, such as macrophages in artery walls that have been overloaded with fats from ingested oxidized LDL particles. Following that, these fats are either returned to LDL particles or transferred to other places, such the liver, for elimination. It is frequently used as a biomarker to predict heart attacks and other cardiovascular illnesses [9]. White blood cells are less likely to become fat-overloaded, change into foam cells, die, and contribute to progressive arteroma when Apo A1 helps remove fats, including cholesterol, from artery walls [10].
It has been discovered that cardiac troponins can predict significant adverse cardiovascular events and have a high sensitivity and specificity for myocardial damage [11]. A serious cardiovascular condition, changed cardiac troponins are frequently seen in patients going through a crisis with diabetes. Few published studies have examined the prognostic importance of this shift in individuals experiencing diabetic crises, despite the fact that elevated troponin is linked to an increased risk of cardiovascular events in people with hypertension [12]. This discovery may have implications for follow-up and therapy.
Two known modifiable risk factors for cardiovascular disease that coexist are dyslipidemia and diabetes. Although many studies have been conducted on the causes, treatments, and management of hypertension, particularly in Nigeria, there is a dearth of published research on the assessment of these indicators as a combined tool in the prognosis and management of diabetes. This research effort would help to bridge this gap, especially in the eastern part of Nigeria. Apolipoprotein A1 and B are well-established biomarkers for the prediction of dyslipidemia, a risk factor for myocardial infarction and cardiovascular disease [13]. Diabetes and an increased risk of cardiovascular disease are related, and the ApoB/A1 ratio may eventually serve as a predictive marker for cardiovascular disease in diabetes.
Materials And Methods
Study Area
The study was carried out in the diabetic unit of Specialist Hospital Owerri. It is a tertiary health institution involved in providing medical care to individuals with hypertension and is located along Hospital road in Umuguma Owerri, Imo state.
Ethical approval.
The ethical approval of Federal Teaching Hospital Owerri was gotten and
Informed consent was also obtained from prospective participants.
Subject Selection and Selection Criteria
One hundred (100) subjects of both sexes between the ages of forty to seventy years and who had fasting blood glucose 200mg/dl or above attending the diabetic clinic of Federal University Teaching Hospital, Owerri was recruited for the study.
One hundred people living with diabetes subjects diabetes and 100 control subjects who were staff of the hospital and whose fasting blood sugar were below 100mg;dl served as the control group.
Inclusion Criteria
The subjects were selected based on the criteria that:
a. They were people living with diabetes subjects who have been attending clinic for at least three months
b. The were within the age of 40 to 70 years.
c. They gave consent.
Exclusion Criteria
The study excluded:
a. Those who refused to give consent.
b. Those who are living with diabetes and severely ill.
c. Pregnant women.
d. Those subjects below forty years and above seventy years of age.
e. Alcoholics, smokers and those on any other type of medication.
Sample Collection
a.Collection of Blood Sample
The study subjects fasted overnight within an interval of eight to twelve hours prior to collection of sample, 5ml of blood was collected aseptically from each subject by venipuncture of the antecubital vein using sterile syringe and needle. The blood sample was placed in a clean plain dry tube, allowed to clot, retracted and centrifuged at 3000rpm for 10 minutes using wisperfuge (model 1384) centrifuge (Sampson, Holland) after which the serum sample was obtained.
The serum was separated using a pasteur pipette and placed in another dry plain tube for the estimation of troponins I, T and C, Apolipoprotein B and A1. All samples were stored at - 20oc prior to analysis.
Laboratory Procedures
- Determination of Troponin I.
This was determined using Enzyme linked immunosorbent assay technique as modified by Assay Genie (Dublin, Ireland) (catalogue number HUES01810)
b. Determination of Troponin T
This was determined using Enzyme linked immunosorbent assay technique as modified by Assay Genie (Dublin Ireland) (catalogue number HUF100262)
C. Determination of Apolipoprotein B (APOB)
This was determined using Enzyme linked immunosorbent assay technique as modified by Assay Genie (Dublin Ireland) (catalogue number HUF100262)
D. Determination of Apolipoprotein A-1 (APO A-1)
This was determined using Enzyme linked immunosorbent assay technique as modified by Assay Genie (Dublin Ireland) (catalogue number HUP104262)
Statistical Analysis
Data was analyzed using software statistical package for social sciences (SPSS) version 21, windows 9.
Difference in mean values between two groups were assessed using student t-Test while difference in mean values between three groups was assessed using one- way analysis of variance (ANOVA). The level of statistical significance was set at P = 0.05 (95% confidence interval). Tests with a probability value of P<0>
Result

Discussions
Troponin 1 and T levels were considerably higher in the treated diabetics than in the control group in this study. Furthermore, there was no appreciable variation in troponin 1 and T levels between those with diabetes and those without [14]. Because cardiac myopathies cause troponins 1 and T to leak into the bloodstream, the study population's noticeably higher levels of these biomarkers may be indicative of sub-clinical cardiac necrosis, which may predict the risk of developing a number of cardiovascular conditions, such as myocardial infarction and stroke, in diabetics. This is in line with a study by [15] that found a significant increase in those biomarkers in those individuals.
While the precise causes of the elevation of cardiac troponins in diabetes are unknown, they may be linked to either an increase in adrenergic system activity or the activation of cardiomyocyte apoptosis processes caused by an increase in the load and stretching of the myocardium. The release of heart troponin into the bloodstream indicates either irreversible or reversible myocyte injury. 16].
The observed increase in cardiac troponin levels in the serum compared to those who were Control could have been caused by myocardial infarction conditioned by exposure to high blood pressure, as studies have shown a correlation between diabetes and elevated serum troponin levels [17] and data support this theory. This is consistent with the research by [18], which found a notable increase in those biomarkers in these participants. These pathways are crucial to the etiology of diabetes, so it makes perfect sense that they would have contributed to the rise in cardiac troponin levels in the serum. In a recent large study, elevated serum troponin T levels in healthy subjects were associated with a considerable long-term risk of diabetes. Additionally, among healthy patients without obvious signs of cardiovascular illness, left ventricular hypertrophy was associated with greater troponin T concentrations (>14ng/L) during the 6-year follow-up period [19] Therefore, assessments of troponins 1 and T may be crucial for both identifying patients who are at a high risk of developing diabetes and for outpatient surveillance.
Male research participants had significantly higher troponin T levels than female subjects. Gender differences in heart muscle mass or myocardial mass may affect troponin T concentrations, with men exhibiting higher levels than women.
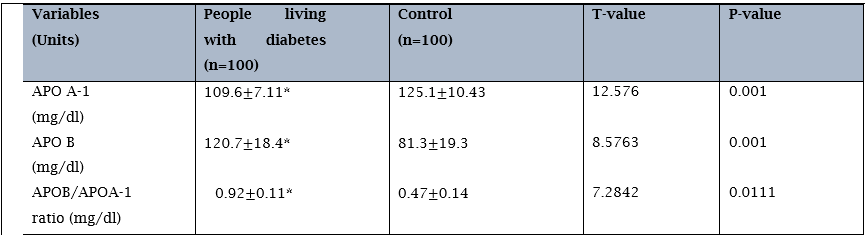
There was a statistically significant decrease in Apolipoprotein A-1 levels and a statistically significant increase in Apolipoprotein B and the ratio of Apolipoprotein B to Apolipoprotein A-1 when comparing diabetes patients to control participants. Neither Apolipoprotein A-1 nor Apolipoprotein B levels were statistically different between individuals with diabetes receiving medication and those who were not; neither Apolipoprotein A-1 nor Apolipoprotein B showed a progressive decrease with age, nor did APO A-1 and B levels between male and female individuals with diabetes during therapy..
Apolipoprotein B, which is the total amount of lipoproteins containing Apo B, is believed to be more accurate in predicting cardiovascular disease than both low and non-high density lipoprotein cholesterol, despite the fact that Apolipoprotein A-1 is known to have an inverse relationship with it. Moreover, the ratio of apo B to apo A-1, which shows the combination of two anterogenic processes, is an even more potent marker of cardiovascular disease [20].
Apolipoprotein B is the primary apolipoprotein chylomicron, very low density lipoprotein, lipoprotein, and low density lipoprotein particles (LDL), and is commonly referred to as the "bad cholesterol" when talking about heart disease and vascular illness in general. LDL is in charge of carrying lipids, fats, and molecules—including cholesterol—to every cell in every tissue in the body [21].
Apolipoprotein B, which is the total amount of lipoproteins containing Apo B, is believed to be more accurate in predicting cardiovascular disease than both low and non-high density lipoprotein cholesterol, despite the fact that Apolipoprotein A-1 is known to have an inverse relationship with it. Moreover, the ratio of apo B to apo A-1, which shows the combination of two anterogenic processes, is an even more potent marker of cardiovascular disease [22]. Apolipoprotein B is the primary apolipoprotein chylomicron, very low density lipoprotein, lipoprotein, and low density lipoprotein particles (LDL), and is commonly referred to as the "bad cholesterol" when talking about heart disease and vascular disease in general. LDL is in charge of carrying lipids, fats, and molecules—including cholesterol—to every cell in every tissue in the body [23]. brought on by high blood pressure, which harms endothelial cells as well [24]. and those with diabetes who have higher levels of apo B are more likely to develop CAD. High levels of apoprotein B may be linked to hypertension through the production of endothelial dysfunction, the rise of coronary artery stenosis, and the infiltration and retention of lipoproteins carrying apo B in the arterial wall [25].
By absorbing fats from inside cells and macrophages in artery walls that have become overloaded with fats from ingested HDL particles, an HDL particle component known as apolipoprotein A-1 helps the efflux of fat molecules. These fats are then transported (in the water outside cells) to other locations, such as back to LDL particles or the liver for excretion [26, 27]. It can therefore predict the onset of cardiovascular disease. More precisely, the ratio of apo B/apo A-1, or LDL and larger particles against HDL particles, has consistently been associated with a higher risk of myocardial infarction. Apolipoprotein A-1 is therefore cardioprotective; however, individuals with diabetes, had much lower levels of this protein than Control. This suggests a higher risk of cardiovascular disease, particularly when apolipoprotein B levels are elevated. This is because the risk of cardiovascular disease is positively and negatively correlated with apo B and apo A1.
References
-
Geddes J, Deans KA, Cormack A, Motherwell D, Paterson K, O’Reilly DS, Fisher BM (2007). Cardiac troponin I concentrations in people presenting with diabetic ketoacidosis. Ann Clin Biochem.;44(Pt 4):391–393.
View at Publisher | View at Google Scholar -
Han Y, Xie H, Liu Y, Gao P, Yang X, Shen Z (2019). Effect of metformin on all-cause and cardiovascular mortality in patients with coronary artery diseases: a systematic review and an updated meta-analysis. Cardiovasc Diabetol. 18(1):1–16.
View at Publisher | View at Google Scholar -
Maack C, Lehrke M, Backs J, (2018) Heart failure and diabetes: metabolic alterations and therapeutic interventions: a state-of-the-art review from the translational research committee of the Heart Failure Association-European Society of Cardiology. Eur Heart J.;39(48):4243–4254.
View at Publisher | View at Google Scholar -
Vander Vorst, E.P. (2020): “High density lipoproteins and Apolipoprotein A1” Vertebrate and invertebrate respiratory proteins, lipoproteins and other body fluid proteins. Subcellular Biochemistry 94(2):399-420.
View at Publisher | View at Google Scholar -
Zhu W, Lai Z, Xue M, Feng S, Feng P, Pan X, Ke X, Chen X, Li Z, Mao H, Yang X, Huang F, Chen W, Xu Y, Li S, Guo Q.(2025) Elevated concentrations of cardiac troponin T are associated with thoracic aortic calcification in non-dialysis chronic kidney disease patients of stage G3 to G5.Ren Fail.;47(1):244
View at Publisher | View at Google Scholar -
Segre CAW, Hueb W, Garcia RMR, Rezende PC, Favarato D, Strunz CMC, (2015). Troponin in diabetic patients with and without chronic coronary artery disease. BMC Cardiovasc Disord. 15(1):72.
View at Publisher | View at Google Scholar -
Xie H, Shen L, Yu P, Wang S, Sun T, Liu X, Wang M, Qian L, Hua J, Chen N, Chen X, Tang S.(2024)Associations of elevated cardiac biomarkers with hyperuricemia and mortality in US adults without prevalent cardiovascular disease.Front Endocrinol (Lausanne). 5;15:1432
View at Publisher | View at Google Scholar -
Agewall S, Giannitsis E, Jernberg T, Katus H (2011). Troponin elevation in coronary vs. non-coronary disease. Eur Heart J. 32(4):404–411
View at Publisher | View at Google Scholar -
Wettersten N, Maisel A (2015). Role of cardiac troponin levels in acute heart failure. Card Fail Rev. 1(2):102–106.
View at Publisher | View at Google Scholar -
Fure B, Bruun Wyller T, Thommessen B (2006). Electrocardiographic and troponin T changes in acute ischaemic stroke. J Intern Med.259(6):592–597.
View at Publisher | View at Google Scholar -
Al-Mallah M, Zuberi O, Arida M, Kim HE(2008). Positive troponin in diabetic ketoacidosis without evident acute coronary syndrome predicts adverse cardiac events. Clin Cardiol. 31(2):67–71.
View at Publisher | View at Google Scholar -
Savonitto S, Morici N, Nozza A, Cosentino F, Perrone Filardi P, Murena E, (2018). Predictors of mortality in hospital survivors with type 2 diabetes mellitus and acute coronary syndromes. Diabetes Vasc Dis Res. 15(1):14–23
View at Publisher | View at Google Scholar -
Eubanks A, Raza F, Alkhouli M, Glenn AN, Homko C, Kashem A, Bove A (2012). Clinical significance of troponin elevations in acute decompensated diabetes without clinical acute coronary syndrome. Cardiovasc Diabetol. 11(1):154–161.
View at Publisher | View at Google Scholar -
Hernández C, Candell-Riera J, Ciudin A, Francisco G, Aguadé-Bruix S, Simó R (2011). Prevalence and risk factors accounting for true silent myocardial ischemia: a pilot case-control study comparing type 2 diabetic with non-diabetic control subjects. Cardiovasc Diabetol. 10(1):9–15.
View at Publisher | View at Google Scholar -
Jensen JK, Atar D, Mickley H (2007). Mechanism of troponin elevations in patients with acute ischemic stroke. Am J Cardiol. 99(6):867–870.
View at Publisher | View at Google Scholar -
James P, Ellis CJ, Whitlock RML, McNeil AR, Henley J, Anderson NE (2000). Relation between troponin T concentration and mortality in patients presenting with an acute stroke: observational study. Br Med J. 320(7248):1502–1504
View at Publisher | View at Google Scholar -
Ozougwu JC, Obimba KC, Belonwu CD, Unakalamba CB(2013). The pathogenesis and pathophysiology of type 1 and type 2 diabetes mellitus. J Physiol Pathophysiol. 4(4):46–57.
View at Publisher | View at Google Scholar -
Raffield LM, Hsu FC, Cox AJ, Carr JJ, Freedman BI, Bowden DW (2015). Predictors of all-cause and cardiovascular disease mortality in type 2 diabetes: Diabetes Heart Study. Diabetol Metab Syndr. 7(1):58.
View at Publisher | View at Google Scholar -
Welsh P, Preiss D, Hayward C, (2020) The biomarkers for acute myocardial infarction and heart failure. Biomed Res Int. 17(2020):2754–2764.
View at Publisher | View at Google Scholar -
Gottlieb A, Yanover C, Cahan A, Goldschmidt Y (2017). Estimating the effects of second-line therapy for type 2 diabetes mellitus: Retrospective Cohort Study. BMJ Open Diabetes Res Care. 1(5):1.
View at Publisher | View at Google Scholar -
Chaudhury A, Duvoor C, Reddy Dendi VS, (2017) Clinical review of antidiabetic drugs: implications for type 2 diabetes mellitus management. Front Endocrinol (Lausanne);8(6).
View at Publisher | View at Google Scholar -
Ogurtsova K, daRocha Fernandes JD, Huang Y, (2017) IDF diabetes atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 1(128):40–50.
View at Publisher | View at Google Scholar -
Zimmermann M, Bunn C, Namadingo H, Gray CM, Lwanda J (2018). Experiences of type 2 diabetes in sub-Saharan Africa: a scoping review. Glob Health Res Policy.;3(1):25.
View at Publisher | View at Google Scholar -
Zekewos A, Loha E, Egeno T, Wubshet K, Merga Z(2018). Prevalence of diabetes mellitus and associated factors in Southern Ethiopia: a Community Based Study. Ethiop J Health Sci.;28(4):451–460.
View at Publisher | View at Google Scholar -
De Rosa S, Arcidiacono B, Chiefari E, Brunetti A, Indolfi C, Foti DP(2018).. Type 2 diabetes mellitus and cardiovascular disease: genetic and epigenetic links. Front Endocrinol (Lausanne). 9(2).
View at Publisher | View at Google Scholar -
Tang O, Matsushita K, Coresh J, (2019). use of high sensitivity cardiac troponin T and I for risk classification in type 2 diabetes. Diabetes.;68(supplement):1. -25
View at Publisher | View at Google Scholar








