
Research Article | DOI: https://doi.org/IJPHRE-RA-26-03
Trend Analysis and Linearity Determination of Numerous Left Ventricular Strain Parameters in patients with Cardiovascular Risk Factors and Normal Four-Dimensional Ejection Fraction
Abstract
Background:
4Dimensional XStrain speckle tracking echocardiography (4DXStrainSTE) is an ingenious technology which blends the STE information acquired from apical three-chamber (3CH), four-chamber (4CH) and two-chamber (2CH) views rendering an exhaustive delineation of multiple LV strain parameters (MLVSP) in a 3Dimensional domain.
Methods:
We aimed to determine the Trend analysis and Linearity of MLVSP in patients with cardiovascular risk factors (CVRF) employing this tool. 500 adult Indian participants (18-60 years of both the sexes) were classified into: Healthy (Group A - n 152) and CVRF group (Group B - n 348). CVRF group was segregated into three categories (Risk category- 1, 2 & 3) based upon increment in risk factors. Nine strain parameters were estimated. The quintessential inclusion criteria for the participants were a 4Dimensional left ventricular ejection fraction (4D-LVEF) of > 50%.
Results:
Trend analysis in CVRF group displayed significantly diminishing pattern of values of global longitudinal strain (GLS), global circumferential strain (GCS) at papillary muscle (pap) level and global circumferential strain rate (GCSR) at mitral valve (mv) level and linear reduction of GLS, GCS at pap level, GCSR at mv and pap level and global radial strain rate (GRSR) at mv level (p<0.05 to p<0.01).
Conclusions:
To our knowledge this is the first research study to investigate the Trend analysis and Linearity in CVRF group on MLVSP utilizing 4DXStrainSTE.
Introduction:
Contemporarily, determination of GLS by 2Dimensional STE is the most exhaustively researched all over the world [1]. American Society of Echocardiography advocated a GLS value of > - 20 + 2 % to be normal [2]. Three-dimension speckle tracking echocardiography necessitates a single LV apical acquirement, translating into lessened acquirement time alongwith an opportune moment to estimate the entire strain parameters [3]. Conversely, because of inferior quality of temporal and spatial resolution, its tracing caliber is abnormally affected. A stitching artifact maybe created between sub-volumes, because of multiple beat acquisitions, resulting in imperfect analysis of speckle tracking [4, 5].
4DXStrainSTE is an ingenious and unique technology which amalgamates the Tomtec GMBH’s 3Dimensional, 4Dimensional portrayal and BetuelTM computation competencies [6]. Consecutively, this distinctive software blends the STE information acquired from apical three chamber (3CH), four chamber (4CH) and two chamber (2CH) views and eventually rendering an exhaustive delineation of LV strain parameters in a 3D domain This tool depending on superior quality of 2D spatial and temporal resolution, rectifies the varying concerns of full volume 3D STE [7].
Single plane 3D echocardiography is affected by the fragmentation of the 3D STE. Nonetheless, the concomitant image resolution is of average variety compared to 2D imaging [8]. Demarcation of the endocardial and epicardial borders is impaired in 3D speckle tracking echocardiography. Conversely, XStrainTM 4D, devoid of these limitations represents a dependable, relatively cheap and easy to operate modality for estimating strain.
In the recent past multiple studies have demonstrated the influence of CVRF on GLS [9, 10]. It is noteworthy that majority of these studies were performed utilizing 2Dimensional STE. However, after exhaustive literature search, we could not encounter any study, where 4DXStrainSTE was employed for determination of Trend analysis and Linearity in MLVSP in the CVRF group. Hence, we embarked on this subject with the aim to thoroughly illustrate the above-mentioned theme by employing 4DXStainSTE.
Method:
Study Design: This is an original research, which was performed over a span of 28 months (September 2021 to December 2023) at Prakash Heart Station, Lucknow, UP, India. The approval for the research work was obtained from the Institutional ethics committee of Prakash Heart Station,(approval no. IEC/PDC/PHSD/2021:01,02).
Study Population:
This was a single center, observational, prospective research study in which the study population comprised of 500 adult Indian participant age 18-60 years of both sex. This research population was classified into two groups (Figure 1).
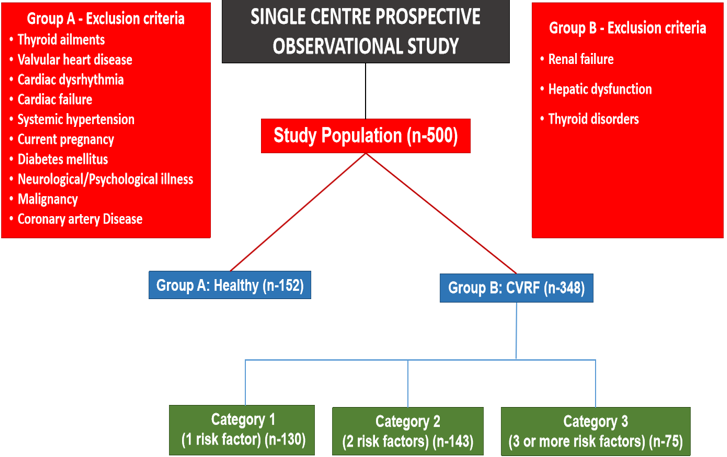
Group A - Healthy Group:
152 healthy individuals aged 18-60 years of both sex, without any cardiovascular risk factors, having a normal resting ECG, 4DXStrainSTE with a 4D-LVEF > 50 % and treadmill stress test (TST) were enrolled.
Group B -Cardiovascular Risk Factor Group
Likewise, about 348 Indian adults of age 18-60 years of both sex with CVRF and in sinus rhythm and 4D-LVEF of > 50% were registered.
The quintessential criteria of this research was that the study participants had a 4D-LVEF of ≥ 50?rived from 4DXStrainSTE.
Clinical evaluation and a thorough medical examination were executed by a cardiac physician. Detailed notes were prepared mentioning the presence of cardiovascular risk factors, if any.
Cardiovascular Risk Factors
- Cardiovascular Disease –
- CAD: previous myocardial infarction, stable/unstable angina, history of acute coronary syndrome and previous percutaneous coronary intervention (PCI)
- CVA (cerebrovascular accident)
- PAD (peripheral arterial disease)
- Diabetes Mellitus
- Hypertension
- Dyslipidemia
- Obesity
- Smoking
Definition of risk factors was in accordance with the current recommendations [11-15].
Echocardiography:
All participants were subjected to a comprehensive assessment of their cardiac functions by conventional transthoracic 2Dimensional echocardiography and 4Dimensional STE. The detailed echocardiographic examination was conducted on the echocardiography system- MY LAB X7 4D XStrain of ESAOTE, ITALY with 1-5 MHZ transducer.
Conventional echocardiography:
Two-dimensional, M-mode, pulse wave doppler (PWD), and continuous wave doppler (CWD) was implemented to estimate the routine parameters of left ventricular (LV) volumes, LV systolic and diastolic functions, LV Mass, LV ejection fraction (LVEF %), cardiac output (CO), cardiac index (CI) early diastolic velocity (E), late diastolic velocity (A) and E/A ratio. Moreover, tissue doppler imaging (TDI) was accomplished and early diastolic myocardial relaxation velocity (E ') and E/E ‘ratio was assessed.
4Dimensional XStrain Echocardiography:
Image Acquisition
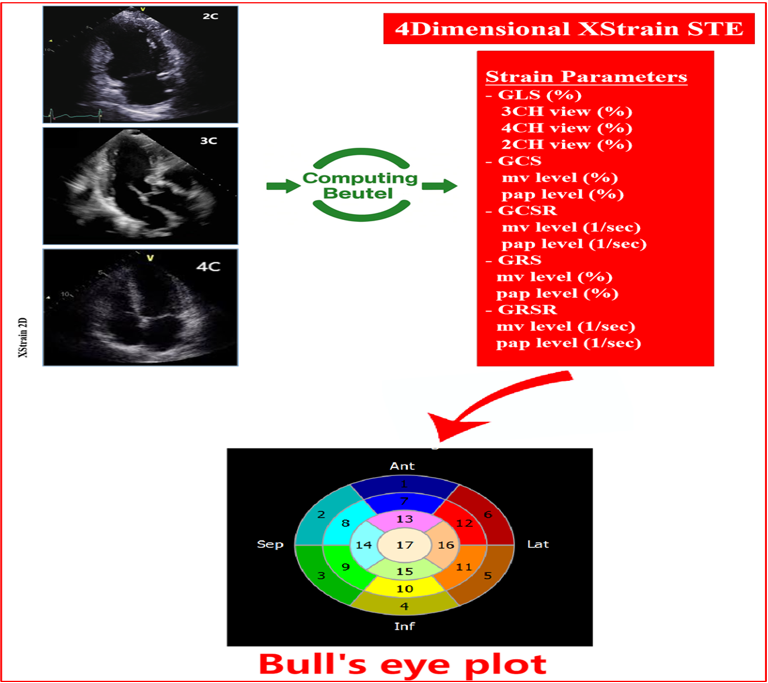
Apical 4CH, 3CH, 2CH and short axis (SX) views at the level of mitral valve (mv) and papillary muscles (pap) were acquired (Figure 2). A minimum of three cardiac cycles were acquired of each one loop with a frame rate of 40-75 frame per second (FPS) and stored digitally on a hard disk for offline analysis.
Offline analysis of acquired images:
Offline speckle tracking analysis was rendered employing XStrain-4DTM (Esaote), software package [16]. LV endocardial and epicardial borders were traced by 13 equidistant tracking points aligned automatically, navigated and supervised by border segmentation tool- AHS (Aided Heart Segmentation, Esaote) [16].
The paramount function of the Beutel Software - XStrainTM 4D is to blend the knowledge from 2D apical 3CH, 4CH and 2CH views and create a 3D/4D reconstruction to automatically furnish values of LV strain data [16]. A 17 segment model Bull’s eye plot was generated displaying the values of LV strain.
Strain Parameters derived from XStrain 4DSTE
GLS (%)
- 3CH view (%)
- 4CH view (%)
- 2CH view (%)
GCS
- mv level (%)
- pap level (%)
GCSR
- mv level (1/sec)
- pap level (1/sec)
Global radial strain (GRS)
- mv level (%)
- pap level (%)
Global radial strain rate (GRSR)
- mv level (1/sec)
- pap level (1/sec)
GLS and GCS are allocated negative value while GRS is nominated with positive values. Similarly, strain and strain rate are earmarked % and 1/sec, respectively.
Statistical Analysis
The enrolled study subjects were classified into Healthy group A and CVRF group B. Additionally, cardiovascular risk factor group was further categorized into:
- Category 1
- Category 2
- Category 3
depending on the presence of one risk factor, two risk factors or three or > three risk factors.
The statistical analysis was performed employing the standard software package - Microsoft excel (R) - Excel 2019, Microsoft corporation, Seattle, Washington, USA. Shapiro Wilk test was used to evaluate the normality of distribution for the continuous variables. The variables having normal distribution were displayed as mean + standard deviation. The calculation of 95 % confidence interval of mean was also rendered.
Statistical significance of dissimilarity between various datasets was estimated by student’s t test for independent groups. Multiple linear regression for determination of linearity or non linearity, Kruskal-wallis test for Trend analysis and displaying their graphs was achieved. The level of significance used was <0>0.05.
Results:
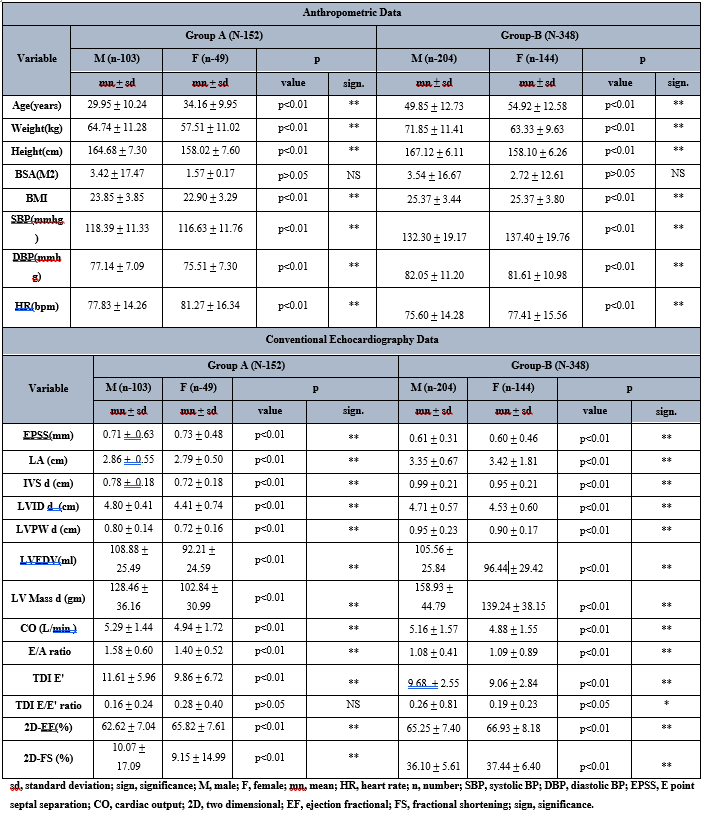
Demographic data
In Group A (Table 1), there were 152 healthy subjects (male 103, female 49) and the age of males and females was 29.5 + 10.24 years and 34.16 + 9.95 years, respectively, suggesting that females were having significantly higher age when compared to males (p<0>
On scrutinizing the anthropometric data of Group B, there were 348 participants amongst which males were 204 and females were 144. The age of males was 49.85 + 12.73 years and of females was 54.92 + 12.58 years. The weight, height, BMI, and diastolic BP (DBP) of men was significantly greater than women (p<0>
Conventional Echocardiography Data
The conventional echocardiographic data was obtained by routine two dimensional echocardiographic.
In males of Group A (Table 1), the left atrium size, IVSd, LVID d, LVPW d, LVEDV, LV Mass d, CO, mitral E/A ratio, LV lateral wall TDI E ' and 2D-FS values were higher than females (p<0>0.05, p<0>
On appraisal of Group B conventional echocardiographic data there were 204 male subjects and 144 females subjects. EPSS, IVSd, LVIDd, LVPWd, LVEDV, LV Mass d, CO, TDI E ' and TDI E/E ' ratio values were greater in men in comparison to women (p<0>
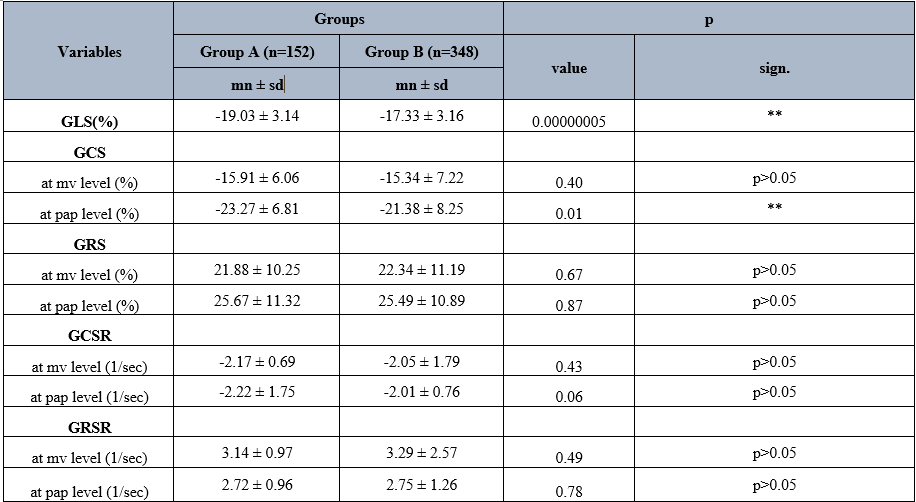
Comparison of 4Dimensional XStrain speckle tracking data of Group A and Group B
LV Strain Data
On comparing the LV Strain data between Group A and B (Table 2), the levels of GLS and GCS at pap level were significantly lower in Group A (p<0>0.05). On the contrary insignificant higher levels of GRSR at mv and pap level were present in Group B (p>0.05).
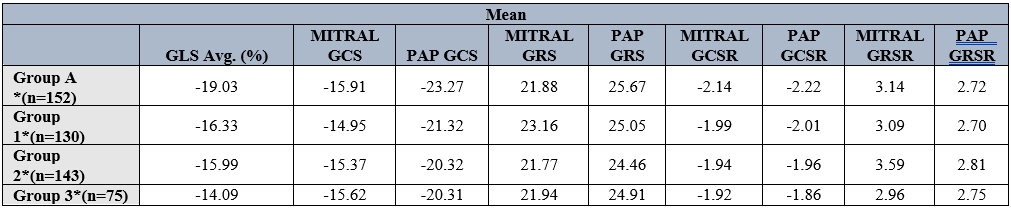
Trend analysis of MLVSP:
On determination of Trend analysis of MLVSP with increasing risk categories (Table 3, 4, Figure 3), there was significantly diminishing pattern of values of GLS, GCS at pap level and GCSR at mv level with increasing risk categories (p<0>0.05).
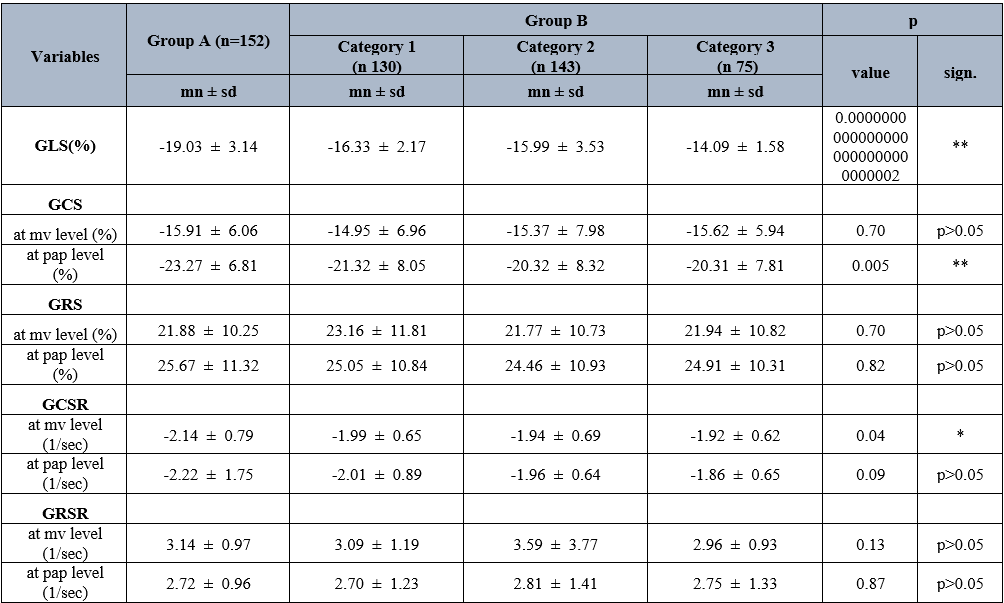
sd, standard deviation; sign, significance; *, significant; **, highly significant; GLS, global longitudinal strain; GCS, global circumferential strain; GRS, global radial strain; GCSR, global circumferential strain rate; GRSR, global radial strain rate; mv, mitral valve; pap, papillary muscle
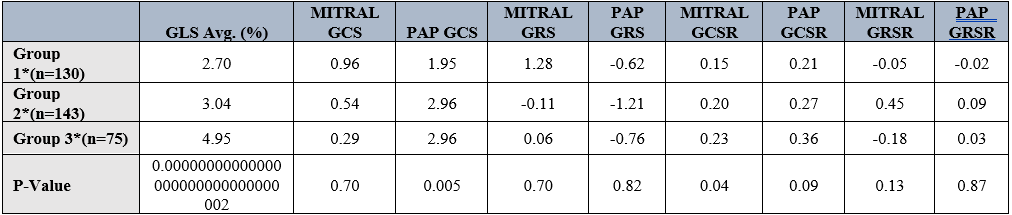
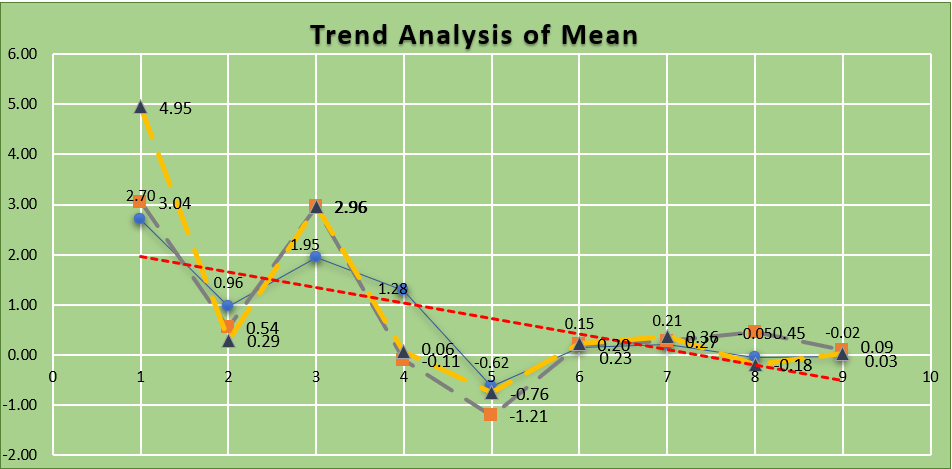
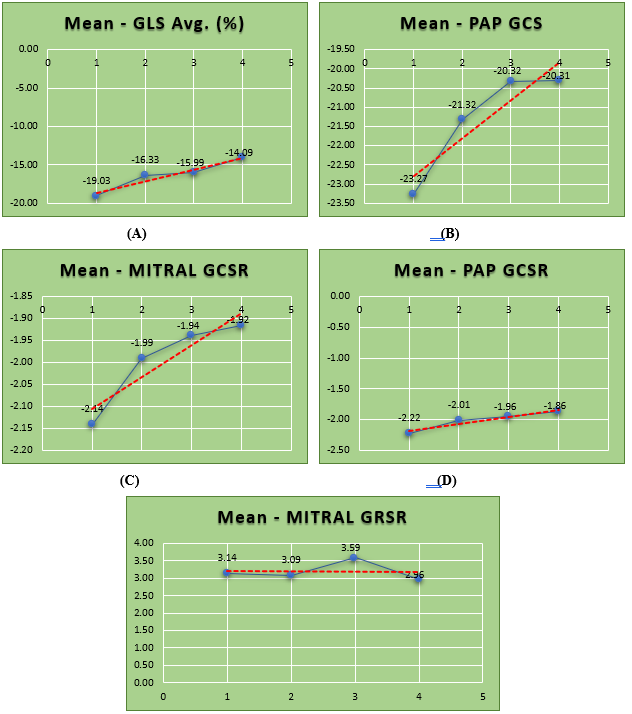
Linearity determination with increasing risk categories:
Figure 4 exhibits linear reduction of mean GLS, mean GCS at pap level, mean GCSR at mitral and pap level and mean GRSR at mv level with increasing risk category (p<0>0.05, p>0.05. p<0>
Discussion:
2D STE is consistently utilized all over the world, owing to the fact that it has the incredible capability to non-invasively evaluate the LV systolic functions and also to analyse LV strain, volumetric and rotational (twist, torsion, rotation) mechanics [16, 17]. However, 2D, 3D and 4D STE is afflicted by several inherent limitations [17]. In the recent past an advanced version of XStrainTM 4D has been employed for superior appraisement of contractile properties of LV [17].
Nevertheless, this advanced technique has not been thoroughly utilized in clinical practice and its outstanding evaluation of deformation, rotational and volumetric mechanics remains underutilized, currently.
4Dimensional / Realtime 3Dimensional / 3Dimensional versus 2Dimensional Echocardiography
Earlier research publications have illustrated the supremacy and accuracy in quantification of LVEF% and LV strain employing realtime three-dimensional (RT3DE) or 4Dimensional echocardiography in comparison to 2Dimensional echocardiography [18-20]. Superiority of these techniques is due to the 2D- LVEF ?rivation being based on geometric assumptions [21].
More importantly, a couple of authors [22, 23] have made noteworthy observations that LVEF % and LV volumes were significantly higher by 2D echocardiography in comparison to RT3DE/4Dimensional echocardiography. We have conducted our research study applying 4DXStrainSTE, which estimates 4DLVEF % and LV volumes in a 3D/4D domain. Earlier studies of Takahashi et al [9] and STAAB cohort study [24] studied the impact of CVRF on LV strain engaging 2Dimensional echocardiography. Perhaps, there was limitations in the accuracy of their projected strain values due to utilization of 2D echo system.
Impact of Cardiovascular risk factors on LV strain parameters:
CVRF are frequently encountered in the elderly population, and if they are not addressed promptly then may cause cardiovascular disease (CVD) [25]. Consequently, the impact of multiple CVRF may lead to subclinical myocardial dysfunction [26]. An aberration in GLS in individuals with preserved LVEF has been previously documented [27] and it has been shown that risk factors could be a marker of early LV dysfunction [9]. Importantly, several studies have reported that the cardiovascular mortality increases with the presence of multiple CVRF [28, 29]. Interestingly, only few studies have been published in the recent past which have aimed to study the influence of CVRF on strain parameters in adults by 2D STE [24, 9].
In a retrospective report of Takahashi et al [9] and STAAB cohort study [24] primarily GLS was the only strain parameter estimated by 2Dimensional speckle tracking echocardiography (2DSTE) systems. In the current research LV strain analysis was achieved by 4DXStrainSTE, the superiority of which has been already established [7, 30]. Our study revealed significantly lower values of GLS and GCS at pap level in CVRF group in comparison to Healthy group (p<0>
Furthermore, we assessed the Trend Analysis, which displayed significantly diminishing pattern of values of GLS, GCS at pap level and GCSR at mv level with increasing risk categories (p<0>0.05). Additionally, Linearity estimation exhibited linearity reduction of values of GLS, GCS at pap level, GCSR at mv and pap level and GRSR at mv level with increasing risk category (p<0>0.05, p>0.05. p<0>
Conclusion:
In the current research we have demonstrated extensive normative data on LV strain parameters in healthy Indian adults and patients with CVRF, utilizing 4DXStrainSTE. On determining the consequences of overall CVRF on LV strain the study showed lower values of GLS and GCS at pap level, (p<0>0.05). On the contrary insignificant higher levels of GRSR at mv and pap level were present in CVRF group (p>0.05).
Moreover, trend analysis of LV strain parameters with increasing risk category revealed significantly diminishing pattern of values of GLS, GCS at pap level and GCSR at mv level with increasing risk categories (p<0>0.05). Furthermore, there was linear reduction of mean GLS, mean GCS at pap level, mean GCSR at mitral and pap level and mean GRSR at mv level with increasing risk categories (p<0>0.05, p>0.05. p<0>0.05).
To our knowledge this is singular research in the world in which 4DXStrainSTE was employed for comprehensively portraying the Trend analysis and Linearity of multifold LVSP in patients with CVRF. Additionally, the consequences on LV strain parameters on CVRF risk group was correlated with healthy group. The novel technology of XStrain 4D STE is relatively cheap and immensely valuable in generating new understanding of the intricate ventricular motion and is highly beneficial in determining the values of GLS and other multifold LV strain parameters.
Limitation of the present research
- This study was single center research in healthy Indian adult subjects and therefore, the normal reference values of this study cannot be considered to be similar to the other ethnic groups: Africans, Europeans, Americans etc.
- The ultrasound machine utilized has an important relevance for the assessment of numerous parameters of LV strain. The values obtained by one system may differ from the other echocardiography unit because of dissimilar software algorithm employed for tracing the endocardium [31].
- Another worrisome limitation is the non-standardization of GLS values spanning throughout different vendors, because of which the strain values will be altered [32, 33].
- Furthermore, the study was not validated against MRI, which is considered to be the gold standard for strain measurements
References
-
Yingchoncharoen T, Agarwal S, Popovic ZB. Normal ranges of left ventricular strain: a meta-analysis. J Am Soc Echocardiogr. 2013; 26:185-91.
View at Publisher | View at Google Scholar -
Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, Flachskampf FA, Foster E, Goldstein SA, Kuznetsova T, Lancellotti P, Muraru D, Picard MH, Rietzschel ER, Rudski L, Spencer KT, Tsang W, Voigt JU. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015; 28:1-39.
View at Publisher | View at Google Scholar -
Jasaityte R, Heyde B, D'Hooge J. Current state of three-dimensional myocardial strain estimation using echocardiography. J Am Soc Echocardiogr.2012; 26:15-28.
View at Publisher | View at Google Scholar -
Papademetris X, Sinusas AJ, Dione DP, Duncan JS. Estimation of 3D left ventricular deformation from echocardiography. Med Image Anal. 2001; 5: 17-28.
View at Publisher | View at Google Scholar -
Elen A, Choi HF, Loeckx D. Three-dimensional cardiac strain estimation using spatio-temporal elastic registration of ultrasound images: a feasibility study. IEEE Trans Med Imaging 2008; 27:1580-91.
View at Publisher | View at Google Scholar -
Muraru D, Niero A, Zanella HR, Cherata D, Badano LP. Three-dimensional speckle-tracking Echocardiography: Benefits and limitations of integrating myocardial mechanics with three-dimensional imaging. Cardiovasc. Diagn. Ther, 2018; 8: 101- 117.
View at Publisher | View at Google Scholar -
Takahashi K, Naami GA. Thompson R, Inage A, Mackie AS, Smallhorn JF, Normal rotational, torsion and untwisting data in children, adoledcents and young adults. J Am Soc Echocardiogr.2010; 23:286-93.
View at Publisher | View at Google Scholar -
Muraru D, Cucchini U, Mihăilă S, Miglioranza MH, Aruta P, Cavalli G, Cecchetto A, Padayattil-Josè S, Peluso D, Iliceto S, Badano LP. Left ventricular myocardial strain by three-dimensional speckle-tracking echocardiography in healthy subjects: reference values and analysis of their physiologic and technical determinants. J Am Soc Echocardiogr. 2014; 27:858-871.
View at Publisher | View at Google Scholar -
Takahashi T, Kusunose K, Zheng R, Yamaguchi N, Hirata Y, Nishio S, Saijo Y, Ise T, Yamaguchi K, Yagi S, Yamada H, Soeki T, Wakatsuki T, Sata M. Association between cardiovascular risk factors and left ventricular strain distribution in patients without previous cardiovascular disease. J Echocardiogr. 2022;20:208-215.
View at Publisher | View at Google Scholar -
Al Saikhan L, Park C, Hardy R, Hughes A. Prognostic implications of left ventricular strain by speckle-tracking echocardiography in population-based studies: a systematic review protocol of the published literature. BMJ Open 2018;8:e023346.
View at Publisher | View at Google Scholar -
Unger T, Borghi C, Charchar F, Khan NA, Poulter NR, Prabhakaran D, et al. International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension. 2020:751334-1357.
View at Publisher | View at Google Scholar -
National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Pane III) final report. Circulation. 2002;106:3143-421.
View at Publisher | View at Google Scholar -
WHO expert consultation. Appropriate body- mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004:363157-63.
View at Publisher | View at Google Scholar -
American Diabetes Association. Standards of Medical Care in Diabetes-2020. Diabetes Care. 2020:43S1-S212.
View at Publisher | View at Google Scholar -
Marston L, Carpenter JR, Walters KR, Morris RW, Nazareth I, White IR, Petersen I. Smoker, ex-smoker or non-smoker? The validity of routinely recorded smoking status in UK primary care: a cross-sectional study. BMJ Open. 2014;4:e004958.
View at Publisher | View at Google Scholar -
MehrotraA, Kacker S, Shadab M, Chandra N, Singh AK. 4Dimensional XStrain speckle tracking echocardiography: comprehensive evaluation of left ventricular strain and twist parameters in healthy Indian adults during COVID-19 pandemic. American Journal of Cardiovascular Disease. 2022;12:192-204.
View at Publisher | View at Google Scholar -
Mehrotra A, Mehrotra A and Shaban M et al. Four-Dimensional XStrain Echocardiographic Assessment of Left Ventricular Strain and Rotational Mechanics: Technology, Clinical Applications, Advantages and Limitations. CVIA. 2024:9.
View at Publisher | View at Google Scholar -
Chen R, Wu X, Shen LJ, Wang B, Ma MM, Yang Y, et al. Left ventricular myocardial function in hemodialysis and nondialysis uremia patients: A three-dimensional speckle-tracking echocardiography study PLoS One. 2014;9:e100265.
View at Publisher | View at Google Scholar -
Zhu M, Streiff C, Panosian J, Zhang Z, Song X, Sahn DJ, et al. Regional strain determination and myocardial infarction detection by three-dimensional echocardiography with varied temporal resolution. Echocardiography 2015; 32:339-348.
View at Publisher | View at Google Scholar -
Jenkins C, Bricknell K, Hanekom L, Marwick TH. Reproducibility and accuracy of echocardiographic measurements of left ventricular parameters using real-time three-dimensional echocardiography. J Am Coll Cardiol 2004;44:878-886.
View at Publisher | View at Google Scholar -
Chen R, Zhu M, Sahn DJ, Ashraf M. Non-Invasive Evaluation of Heart Function with Four-Dimensional Echocardiography. PLOS ONE. 2016;11: e0154996.beim
View at Publisher | View at Google Scholar -
Patted SV, Ambar S, Porwal SC, Halkati PC, Prasad MR, Metgudmath VB, Hesarur V, Patil V, Kumar MA, Chitrali S. Comparison of left ventricular volume and left ventricular ejection fraction by 2-dimensional echocardiography by Simpson's method & real time 3-dimensional echocardiography in patients of normal conduction with normal left ventricular function, complete left bundle branch block with normal left ventricular function and with left ventricular dysfunction, Journal of Indian College of Cardiology. 2018;8:167-171.
View at Publisher | View at Google Scholar -
Ali Al-Allak HM, Noaman Al-Aboodi AH. A Four-Dimensional Volumetric Quantification of the Left Ventricle in Healthy Pregnant Women in the Third Trimester. Cureus. 2023;15:e46342.
View at Publisher | View at Google Scholar -
Morbach C, Walter BN, Breunig M, Liu D, Tiffe T, Wagner M, Gelbrich G, Heuschmann PU, Störk S; STAAB consortium. Speckle tracking derived reference values of myocardial deformation and impact of cardiovascular risk factors - Results from the population-based STAAB cohort study. PLoS One. 2019;14:e0221888.
View at Publisher | View at Google Scholar -
Matsuoka M, Inoue T, Shinjo T, et al. Cardiovascular risk profile and frailty in Japanese outpatients: the Nambu Cohort Study. Hypertens Res. 2020;43:817-823.
View at Publisher | View at Google Scholar -
Lloyd-Jones DM, Braun LT, Ndumele CE, et al. Use of risk assessment tools to guide decision- making in the primary prevention of atherosclerotic cardiovascular disease: a special report from the American Heart Association and American College of Cardiology. Circulation. 2019;139:e1162-e1177.
View at Publisher | View at Google Scholar -
Edvardsen, Thor & Helle-Valle, Thomas & Smiseth, Otto. Systolic Dysfunction in Heart Failure with Normal Ejection Fraction: Speckle-Tracking Echocardiography. Progress in cardiovascular diseases. 2006;49:207-14
View at Publisher | View at Google Scholar -
Li D, Jia Y, Yu J, et al. Adherence to a healthy lifestyle and the risk of all-cause mortality and cardiovascular events in individuals with diabetes: the ARIC study. Front Nutr. 2021;8: 698608.
View at Publisher | View at Google Scholar -
Barr EL, Zimmet PZ, Welborn TA, et al. Risk of cardiovascular and all-cause mortality in individuals with diabetes mellitus, impaired fasting glucose, and impaired glucose tolerance: the Australian Diabetes, Obesity, and Lifestyle Study (AusDiab). Circulation. 2007;116:151-7.
View at Publisher | View at Google Scholar -
Van mil AC, Pearson J, Drane AL, Cockcroft JR. McDonnell B and Stoehr EJ. Interaction of LV Twist with arterial haemodynamics during localised. Exp Physiol. 2016; 101:509-520.
View at Publisher | View at Google Scholar -
Patrianakos, AP, Zacharaki AA, Kalogerakis A et al. Two-dimensional global and segmental longitudinal strain: are the results from software in different high-end ultrasound systems comparable?. Echo Res Pract 2015;2:29-39.
View at Publisher | View at Google Scholar -
Nelson MR, Hurst RT, Raslan SF, Cha S, Wilansky S and Lester SJ. Echocardiographic measures of myocardial deformation by speckle tracking technologies: the need for standardization? J Am Soc Echocardiogr 2012;25:1189-1194.
View at Publisher | View at Google Scholar -
Thomas JD and Badano LP. EACVI-ASE-industry initiative to standardize deformation imaging: a brief update from the co-chairs. Eur Heart J Cardiovasc Imaging 2013;14:1039-1340.
View at Publisher | View at Google Scholar








