
Research Article | DOI: https://doi.org/IJCCRI-RA-24-009
The Estimation of Copper Serum Level Among Obese Children
Abstract
Background: Obesity means an excess amount of body fat. No general agreement exists on the definition of obesity in children as it does adults. Most professionals use published guidelines based on the body mass index (BMI), or a modified BMI for age, to measure obesity in children. Others define obesity in children as body weight at least 20% higher than a healthy weight for a child of that height, or a body fat percentage above 25% in boys or above 32% in girls
Objective: to estimate the serum level of copper among obese children.
Methods: This comparative study was conducted on fifty of overweight and/or obese children (based on BMI) and thirty of clinically healthy, age and sex matched children's served as controls also, the cases and controls were selected randomly from the pediatrics outpatient clinic of Benha University Hospital and Sheben El Kom Educational hospital, in the period between 2013 to 2015. Parental consent was obtained for all children included in the study.
Results: In the current study there were no significant difference found between patients and control group regarding age, sex and residence, but there was significant difference between the two groups regarding income and socioeconomic state. P=0.04. Also, there were no static difference in height in patient when compared to control group, and patients had a higher statically significant Weight, BMI and Skin fold thickness when compared to control group. Additionally, that there were significantly higher rate of frequent bad nutritional habits including shipping breakfast (p=0.022) consumption of energy- dense food and food consumption during TV watch in patients than controls. P< 0.001 and the children's physical activity levels were lower in the patient’s group than the control group. P<0.001.
Conclusion: The obesity varied remarkably with different socioeconomic levels. Obese children had a characteristic nutritional pattern like skipping breakfast and consumption of energy dense food.
Introduction:
Obesity means an excess amount of body fat. No general agreement exists on the definition of obesity in children as it does adults. Most professionals use published guidelines based on the body mass index (BMI), or a modified BMI for age, to measure obesity in children. Others define obesity in children as body weight at least 20% higher than a healthy weight for a child of that height, or a body fat percentage above 25% in boys or above 32% in girls (Robert, 2006).
Children with BMI-percentile-for-age between 85th and 95th percentile are overweight and children at or above the 95th percentile are considered obese. Obesity has a profound effect on a child's life. It increases the child's risk of numerous health problems, and it also can create emotional and social problems. Obese children are also more likely to be obese as adults, increasing their risk of serious health problems such as cardiovascular complications (American Obesity Association Centers for Disease Control and Prevention; "Childhood Overweight": 2006).
Copper is an essential trace element for humans and animals. In the body, copper shifts between the cuprous (Cu1+) and cupric (Cu2+) forms, though most of the body's copper is in the Cu2+ form. The ability of copper to easily accept and donate electrons explains its important role in oxidation reduction reactions and acts as antioxidants in scavenging free radicals (Victoria, 2007). Excess weight associated with lipid metabolism disturbances might predispose to changes in serum Cu concentrations in obesity indicating a possible mechanism of this mineral, contributing to peroxidation or acting as an antioxidant. It should be emphasized that intracellular reserves of Cu remain unaltered under these conditions. (LIMA et al., 2006)
Obese children and adolescent have an increased risk for CVS complications that include elevation of blood pressure, clustering of CVS risk factors (Metabolic Syndrome), changes to arterial wall thickness (elasticity and endothelium), as well as changes in left ventricular structure and function. Some of these cardiovascular problems may be initiated or potentiated by obstructive sleep apnea that can accompany obesity in children. Many of such changes have been noted to reverse or improve with weight reduction. (Ting Fei Ho, 2009).
Atherosclerosis begins in childhood as deposition of cholesterol and its esters with fatty streaks in the intimae of large muscular vessels, more lipid accumulation may progress seamlessly to fibrous plaques and these plaques might rupture and cause thrombotic arterial occlusion and ischemic damage to vital organs. The earliest stages and progression of atherosclerosis in childhood are influenced by the same major established risk factors for this condition in adults-dyslipidemia, hypertension and diabetes mellitus which is very common with obesity. Controlling these risk factors at any age is beneficial, but the earlier primary prevention begins, the better the result. As recommended by the American Academy of Pediatrics, pediatricians should support both control and prevention of these risk factors in children via lifestyle modification. Drug treatment can be used to supplement lifestyle modification in the few cases of obese children (McGill, 2004). This study aims to estimate the serum level of copper among obese children.
Patients and Methods
This study conducted on fifty of overweight and/or obese children and thirty of clinically healthy, age and sex matched children's served as controls, The cases and controls were selected randomly from the pediatrics outpatient clinic of Sheben El Kom Teaching hospital, in the period between 2021 to 2022. Parental consent was obtained for all children included in the study.
Inclusion criteria: Age ranged from 1 to 14 years, both sexes are included BMI equal or more than 85 percentiles for age and gender based on the Egyptian growth reference charts.
Exclusion criteria: An overweight and obese child with, Endocrinal disorders, Chromosomal and genetic disorders, Cardiovascular disorders, History of drugs intake that increases body weight like steroids therapy.
Every child was subjected to:
Clinical evaluation including Complete medical history including (age, sex, residence and socioeconomic state calculated according to Egyptian score including mother and father education and crowding index (Fahmy and El-Sherbini, 1985), Complete nutritional history, Anthropometric measurements and Clinical examination (chest, heart, abdominal and neurological examination)
Children Body Mass Index: (BMI), calculated as weight in kilograms divided by the square of height in meters) and the children were classified according to specific charts for age and sex.
Skin fold Thickness: The triceps and sub scapular skin fold thickness were measured using skin fold caliper according to American College of Sports Medicine guidelines for skin fold measurement.
Obesity indices: BMI of ≥95th percentile for age and gender (BMI of >30) (whichever is smaller) considered obese. according to The Centers for Disease Control and Prevention (CDC). BMI of ≥85th percentile but <95th>
Laboratory evaluation: Serum levels of copper by atomic absorption spectrophotometer.
Determination of serum level of copper: Two ml of blood were taken from each patient by venipuncture, avoiding hemolysis and contamination. The sample was placed in a water bath for 1 hour, then centrifuged. The sample obtained was stored at -20c.
Technique of estimation of copper: Estimation of serum copper was done according to the method of Brown et al., (1979) while estimation of serum copper was done according to the method of Henary, (1979). This was done by the atomic absorption spectrophotometer model GBC 901.
Radiological assessment including plain X-ray chest and heart posterior-anterior view was performed to detect the presence of cardiomegaly (CT ratio), assessment of pulmonary vasculature and to detect any abnormalities in the lung fields.
Electrocardiography (ECG): Using CARDIMAX FX 7102, to show if there’s evidence of ventricular hypertrophy or pulmonary hypertension
Statistical analysis
Data were fed to the computer and analyzed using IBM SPSS software package version 20.0 (Kirkpatrick et al., 2013). Qualitative data were described using number and percentage. Quantitative data were described using range (minimum and maximum) mean, standard deviation and median. Comparison between different groups regarding categorical variables was tested using the Chi-square test. If it reveals normal data distribution, parametric tests were applied. If the data were abnormally distributed, non-parametric tests were used. for normally distributed data, comparison between the two studied groups were done using independent t-test. Significance of the obtained results was judged at the 5% level (Kotz et al., 2006).
Results
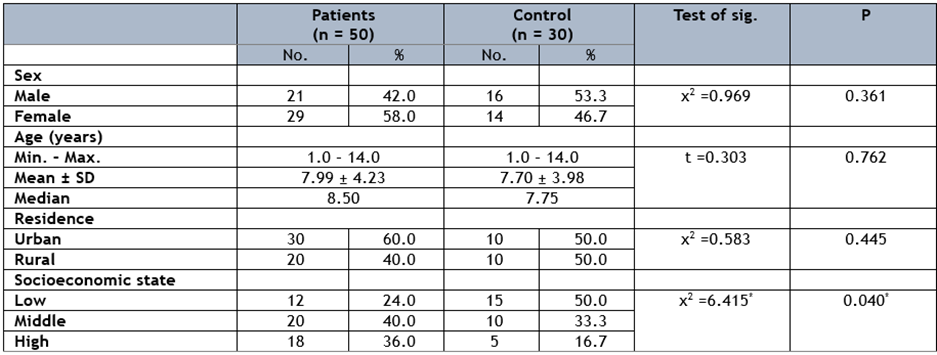
In the current Study there were no significant difference found between patients and control group regarding age, sex and residence, but there was significant difference between the two groups regarding income and socioeconomic state. P=0.040. (table 1).
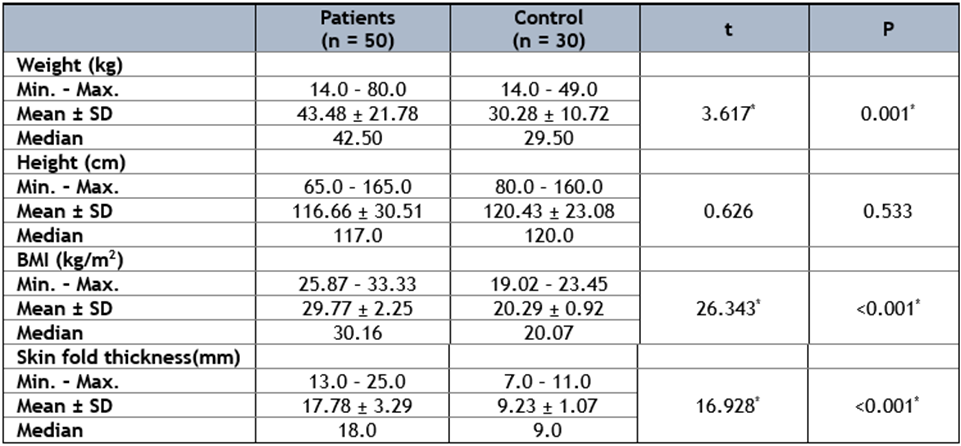
Also, there were no static difference in height in patient when compared to control group, and patients had a higher statically significant Weight, BMI and Skin fold thickness when compared to control group. (Table 2)
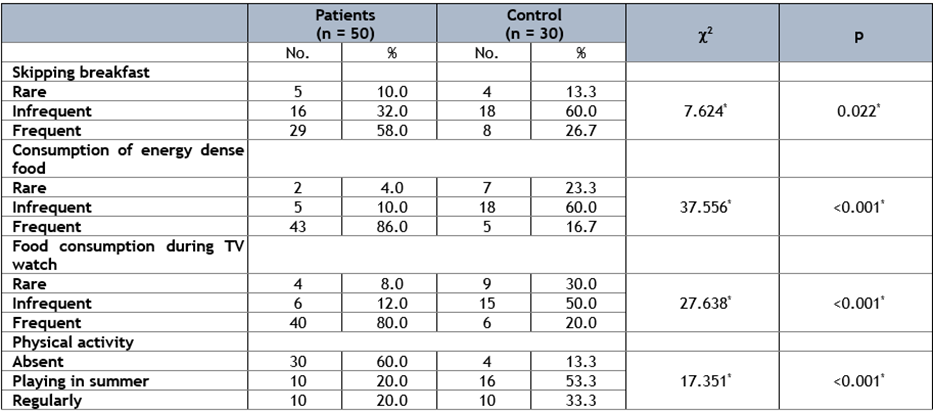
Additionally, that there were significantly higher rate of frequent bad nutritional habits including shipping breakfast (p=0.022) consumption of energy- dense food and food consumption during TV watch in patients than controls. P< 0>
Also, patients had a higher statically significant Serum copper level when compared to control group P < 0>

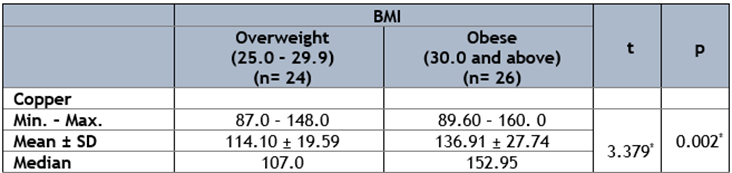
Additionally, there were Statistically significant increase in obese group than overweight group regarding serum copper level, P=0.002. (table 5)
Discussion
Childhood obesity is a public health problem of epidemic proportions with estimates of 1 in 3 children and adolescents classified as overweight or obese (Ogden et al., 2010). The aim of our study was to explore the relationship between nutritional obesity and altered levels of some micronutrients (zinc, copper) and to examine the effect of obesity on cardiovascular system.
In our study there were no significant difference regarding age (P=0.762) and sex (P=0.361) between patients and control groups. We observed increased percentage of obesity in females 58% than in males 42%. Previous study among Greek preschoolers found that no statistical differences in the prevalence of obesity between males and females (Yiannis, 2007). In contrast to our result Stark, (2011) found that there was higher percentage of obesity among males’ children but Canning, (2004) also found increase of prevalence of obesity among girls.
In our study Serum copper level was significantly higher in-patient group compared to that of the control group (p <0 p=0.002).> or = 30 kg/m2) compared to a group of 32 healthy subjects. The authors noted an elevation of serum copper in obese with a middle level of 133 mg/dl significantly superior to the middle level of serum copper of healthy subjects, 108 mg/dl (p < 0> or = 40 kg/m2 showed a high concentration of serum copper although only 5% of obese with BMI < 40 xss=removed xss=removed>
Also, Vitoux et al., (1999) verified that erythrocyte Cu concentrations were higher than the reference value in obese individuals. The assessment of erythrocyte Cu can be considered a safe biomarker, as these cells do not suffer the influence of inflammatory and hormone alterations. Erythrocyte Cu variations occur more slowly, whereas plasma Cu might be influenced by diet and circadian variations. Zwirska-Korczala et al., (2003) reported that the complications of obesity, not only those attributed to the lipid profile and diet but also to Cu disturbances exacerbating the harmful effects of lipoperoxidation. Excess weight has been considered a causal factor of lipid peroxidation and of decreased antioxidant enzymes. This constitutes an alert for possible chronic complications over the course of the disease, given the relation between plasma lipid alterations and lipoperoxidation markers (malondialdehyde) as indicative of oxidant state disorders. Zargar et al., (1998) concluded that in trace element metabolism the best-known interaction is the reported antagonism between zinc and copper. Excessive dietary zinc is reported to induce copper deficiency by several mechanisms, all involving induced synthesis of an intracellular binding protein, metallothionein. Excessive intake of zinc is thought to induce synthesis of the protein, resulting in sequestering of both metals, with subsequent excretion when cells are sloughed into the intestinal lumen. Hormonal influences may also lead to apparently antagonistic zinc copper interactions. Both carbohydrate-active steroids and a mononuclear phagocyte produced hormone, interleukin-1, enhance intracellular zinc accumulation while increasing intracellular copper efflux as caeruloplasmin. The net result of these effects is a decreased plasma concentration of zinc and an increased concentration of copper.
Conclusion
Obesity varied remarkably with different socioeconomic levels. Obese children had a characteristic nutritional pattern like skipping breakfast and consumption of energy dense food. The copper nutritional status in obese individuals is altered and serum zinc is significantly lower in patients than controls and serum copper is significantly higher than controls.
Consent for publication
all authors have read and revised well for the manuscript and agree to publish. Availability of data and material: All data supporting the study are presented in the manuscript or available upon request.
Competing interests
There is no conflict of interest.
Funding:
The author received no financial support for this article's research, authorship, and publication.
References
-
Canning P.M., Courage M.L. and Frizzell L.M.(2004): Prevalence of overweight and obesity in a Provincial population of Canadian preschool children. J, 171(3):240-242.
View at Publisher | View at Google Scholar -
Dambal S.S., Indumati V. and Suchetha K.(2011): Relationship of obesity with micronutrients . International Journal of Applied Biology and Pharmaceutical Technology. ISSN; 0976-4550.
View at Publisher | View at Google Scholar -
Fahmy S.I. and El Sherbini A.F. (1985):Determing simple parameters for social classifications for health research Bull High Institute ,Puplic Health; 13:95-107. Coated from El-Gilany A.H.
View at Publisher | View at Google Scholar -
Lima S.C.V.C., Arrais R.F., Sales C.H. et al. (2006): Assessment of Copper and Lipid Profile in Obese Childrenand Adolescents. Departments of Nutrition, Pediatrics, and Clinical and Toxicologic Analysis, Brazil. 1559-0720/06/114(1–3)–0019
View at Publisher | View at Google Scholar -
McGill H.C., McMahan C.A. and Gidding SS (2004): Contemporary Reviews in Cardiovascular Medicine,Preventing Heart Disease in the 21st Century,Implications of the Pathobiological Determinants of Atherosclerosis in Youth (PDAY) Study University of Texas Health Science Center at San Antonio, USA. hmcgill sfbr.
View at Publisher | View at Google Scholar -
Mezetti A., Pierdomenico S. D., Costantini F. and et al., (1998). Copper/zinc ratio and systemic oxidant load: effect of aging and aging-related degenerative diseases, Free Radical Biol. Med. 25(6), 676–681.
View at Publisher | View at Google Scholar -
Ogden C.L., Carroll M.D., Curtin L.R. and et al. (2010): Prevalence of high body mass index in US children and adolescents, 2007-2008. J Am Med Ass, 303(3), 242-249.
View at Publisher | View at Google Scholar -
Omar S, Abdennebi M., Ben Mami F. and et al. (2001). Serum copper levels in obesity: a study of 32 cases. Tunis Med. Jun-Jul; 79(6-7): 370-3. PMID: 11771433 .
View at Publisher | View at Google Scholar -
Pino C. G., Treche M. H., Ferrer R. S. and et al. (1992). Niveles sericos de cromo, cobre y cinc en un grupo de niños obesos, Rev. Cubana Aliment. Nutr. 6(2), 94–98.
View at Publisher | View at Google Scholar -
Robert ferry J. and Melissa S. (2006). American Obesity Association. Centers for Disease Control and Prevention;
View at Publisher | View at Google Scholar -
Stark M.J., Niederhauser V.P., Camacho J.M. and et al.(2011): Prevalence of overweight and obesity in children at a Health Maintenance Organization in Hawai'i, 3(2):165-87.
View at Publisher | View at Google Scholar -
Ting F.H. (2009), Cardiovascular Risks Associated with Obesity in Children and Adolescents.Ann Acad Med Singapore;38:48-56.
View at Publisher | View at Google Scholar -
Victoria J.Drake, Ph.D. (2007): Micronutrient Information Center, Linus Pauling Institute,Oregon State University april 2007. http://lpi.oregonstate.edu/mic/minerals/zinc,copper.
View at Publisher | View at Google Scholar -
Vitoux D., Arnaud J. and P. (1999): Chappuis, Are cooper, zinc, selenium in erythrocytes valuable biological indexes of nutrition and pathology J. Trace Elements Med. Biol. 13, 113–128.
View at Publisher | View at Google Scholar -
Yiannis M., Vassiliki C., Maria K. and et al. (2007): Prevalence of obesity in preschool Greek children, in relation to parental characteristics and region of residence307(5):483-490.
View at Publisher | View at Google Scholar -
Zargar A. H., Shah N. A., Masoodi S. R. et al. (1998). Copper, zinc, and magnesium levels in non-insulin dependent diabetes mellitus Postgrad Med J 74: 665-668
View at Publisher | View at Google Scholar -
Zwirska-Korczala K., Jochem J. ,Rbus-Kalinowska B. and et al. (2003). Birkner, Assessment of blood superoxide dismutase, glutathione peroxidase activity and malondialdehyde concentration as oxidation status parameters in obese women, Pol. Arch. Med. Wewn. 110(1), 725–731.
View at Publisher | View at Google Scholar








