
Case Report | DOI: https://doi.org/BRCA-RW-24-009
Reemphasizing The Significance of Fertility Preservation in Cancer Patients Needing Chemotherapy And /Or Radiotherapy- A Case Report
Abstract
Having reviewed earlier on how significant it had become to counsel both male and female patients prior to initiation of chemotherapy/radiotherapy to get either cryopreservation of sperm/ oocyte before initiating chemotherapy/radiotherapy with the escalation of 5 year survival rates in cancer survivors thus more of them needing to seek for fertility.However even till now Clinical practitioners fail to do so as emphasized by the case reported here for a male patient who received treatment at the age of 25 for non Hodgkin’s lymphoma;surgery followed by chemotherapy and radiotherapy without any counselling for semen cryopreservation as a result of which their conception was impacted by type II Arnold Chiari malformations ending in MTP.Since patients semen analysis was normal and no prior counselling it was difficult to counsel the husband how this might recur unless precautionary measures but fell on deaf ears.
Introduction:
With the greater advancements in field of cancer treatment, the survival rates have escalated remarkably, thus the need arising for the fertility preservation in the survivors with regards to oocyte/embryo/ovarian tissue / Cortical tissue/ testicular tissue transplantation/ sperm cryopreservation has assumed great importance particularly for those receiving chemotherapy that too with alkylating agents. Furthermore, the need further is enhanced in younger adults along with adolescents diagnosed for cancer and need chemotherapy and are yet to attain puberty where it might not be feasible to do cryopreservation of oocytes. However even in adult cases how significant it has become for any clinical practitioners tackling patients where diagnosis of cancer is made in addition to emphasize the significance of counselling both maleand female patients prior to initiation of chemotherapy/radiotherapy to get either cryopreservation ofsperm/oocytebefore initiating chemotherapy/radiotherapy.We have made numerous publications regarding this issue ,however still we come across akin patients who never received any counselling keeping longterm fertility in mind .The case report we present here highlights this issue .
Case Report
A couple came to our centre on 11/2/2023 with the history of married for 9 yrs along with previously having a conception where antenatally a diagnosis of typeII Arnold Chiari malformations , thereby MTP was performed.Wifes age now was 40 yrs and husband37 yrs. On in depth probing we got the history of husband obtaining treatment for certain axillary mass which was surgically removed in addition to got chemotherapyx 6 cycles and radiotherapy for4 cycles although the nature of chemotherapy was not known he later told diagnosis was non Hodgkin’s lymphoma.This had been done 10yrs previously.Now they had come for counselling for subsequent pregnancy in addition to chances for a normal child later. His RSA displayed a semen count of 70m/ml,with apparently morphology was normal in 70%.. Taking into account there being a history of both chemotherapy along with radiotherapy receipt we counselled her for Intracytoplasmic sperm injection (ICSI)in addition to preimplantation genetic testing( PGT) for aneuploidy(PGT-A) prior to embryo transfer(ET)once normal PGT report attained however the couple were not willing to attribute this problem to chemotherapy along with radiotherapy as wellas RSA was normal they wanted simpler approach.Earlier we had reported innumerable reviews on fertility preservation in both male and female cancer therapy with chemotherapy particular alkylating agents along with considerable research getting performed even in young children in addition to adolescents who have not attained puberty along with any treating physician needs to refer these cases for counselling for fertility preservation as per age either gametes/testicular /ovarian cortical tissue/testicular tissue transplantation[1-5].
Why Need for Fertility Preservation:
Despite the banking of sperm prior to the initiation of cancer treatment is recommended, conditions might be there that prevent the successful cryopreservation of sperm in personalized patients. The restoration of spermatogenesis subsequent to chemotherapy or radiotherapy is acknowledged to be unanticipable as well as studiesof spermatogenesis in long-term cancer survivors have illustrated corroboration of continuation of azoospermia or robust oligospermia in approximately 24% of cases .However, the ultimately resumption of sperm generation inplethora of posttherapy cancer patients incites the query if the posttreatment safety of sperm utilized in natural or via assisted reproductive technologies(ART) on contemplating conception. Choy et al.[ 6], assessed this problem of reproductive safety in addition to the risks of utilizing sperm from cancer patients.
In reference to these botherations over reproductive safety are basically based in the plausible existence of DNA injury stimulated by the germ line chemotherapy or radiotherapy. Chemotherapeutic agents, specifically the alkylating agents which get commonly utilized, might stimulate genetic injury by cross-linking DNA along with introducingsingle-strand DNA breaks; the akin mutagenic actions of radiation originating from DNA fragmentation evoked within cells (2, 6). The estimation of genetic safety depends largely on the spermatogenic stage at which a mutation is attained. In view of down-regulation of DNA repair mechanistic modes which take place in late spermatogenesis,spermatogenic cells further along the differentiation pathway canonically do not possess the capacity of repair DNA injury, nor do they possess the capacity generally ofgoing via total apoptosis [7].Thereby the ejaculated spermatozoa might foster substantial genomic injury which theoretically might get transmitted to a resultant embryo subsequent to fertilization.Fortunately, mutations that stimulate sole stages of spermatogenesis would provide a risk period for thegeneration of genetically endangered sperm that is restricted to approximately 3 months/ the time taken for a full spermatogenic cycle to finish [7]. Conversely, mutations suffered by the spermatogonial stem cells possess the capacity of plausibly healed by inherent DNA repair mechanistic modes or entirely eliminated by the cell's apoptotic machinery. Nevertheless,since these spermatogonial cells which portray the progenitors from which all future germ lines get obtained , any sustaenance ofmutations in these cells dodge repair or depletion will persistently get transmitted, resulting in the plausiblegeneration of mutation-carrying sperm for the full time period of a man's lifetime[7].
There is a scarcityof peer-reviewed literature in reference to reproductive results in the acute, posttreatment duration of time. These studies are clearly restricted in view of ethical along with the practical botherations. Existing studies implicating humansare usually largely removed from the acute, posttreatment time frame, and they previously canonically typically conclude that the frequency ofcongenital anomalies in the children of men earlier having exposure to chemotherapeutic agents is not more compared to that observed among the general population [rev in 6]. Nevertheless, case studies of men who have managed to conceive subsequent to cancer therapy continue to corroborate the plausibility of an association between cancer therapy as well as congenital anomalies in humans, since instances of resultant syndactyly, tetralogy of Fallot, in addition to anencephaly have been revealed [8].
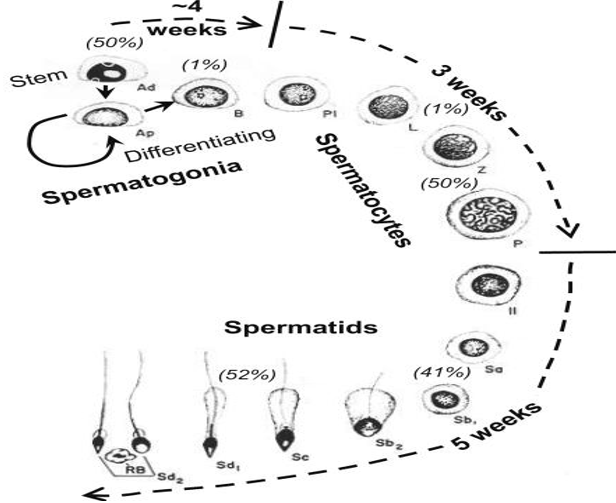
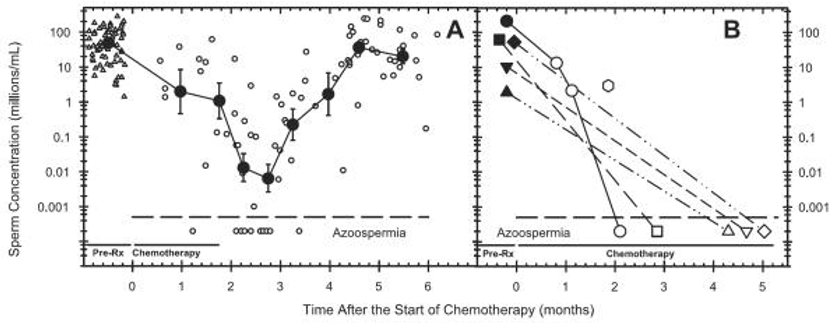
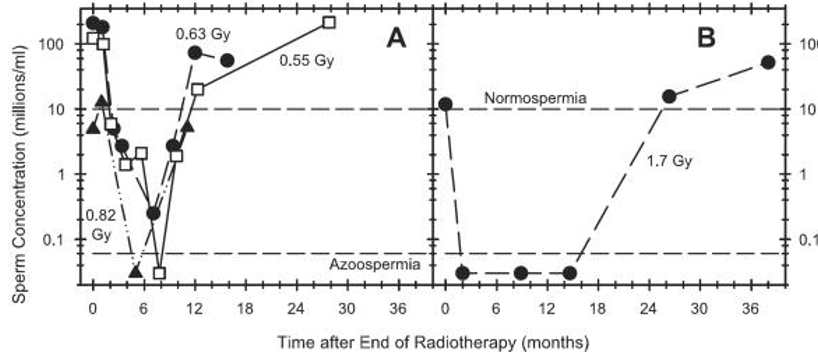
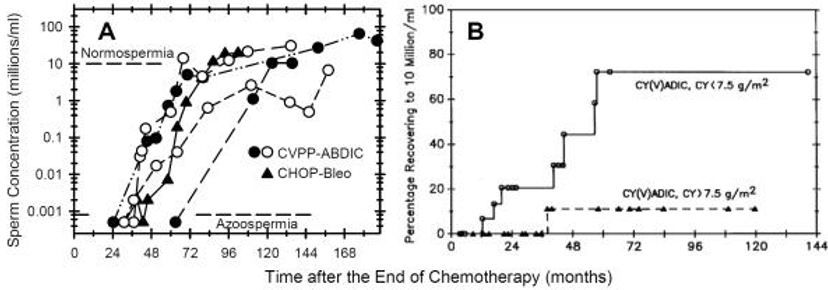
Further Meistrich ML.[9] reviewed the actions of chemotherapy as well as radiotherapy on spermatogenesis in humans.
They described the i)Course of how sperm decrease takes place(Figure1)-see ref no 9 for details.
Conclusion
Thereby our patient received the usual drugs for non Hodgkin’s lymphoma probably in addition to radiotherapy as well as although normal RSA as explained by ChoyJT, BranniganRE their child suffered from typeII Arnold Chiari malformationswhich adds to the list of congenital anomalies earlier documented in the aftermath of receiving chemotherapy and radiotherapy,thereby emphasizing on cryopreservation prior to any chemotherapy and radiotherapy to avoid such effects on the gametes and documentation of these congenital anomalies is significant for convincing the patients in addition to treating clinical practitioners.
References
-
Kulvinder Kochar Kaur, Allahbadia GN, Singh M. An Update on Management of Oncofertility-Does the Use of Vsels Appear Practical in the Near Future in Human Malignancies Replacing Cortical Tissue/Testicular Tissue Transplantation. Int J Stem Cell Regen Med2019; 1(1): 103.
View at Publisher | View at Google Scholar -
Kulvinder Kochar Kaur,Allahbadia GN,Singh M. How Far Have We Reached with Regards to Our Endeavours in Testicular Tissue Transplantation Along with in Vitro Spermatogenesis After Success in Animals - A Systematic Review”. Archives of Urology 2020;3(2):1-15.
View at Publisher | View at Google Scholar -
Kulvinder Kochar Kaur,Allahbadia GN,Singh M. “An update on fertility preservation in men undergoing cancer treatment, irrespective of age-A Comprehensive Review”.JEndocrinol 2020.
View at Publisher | View at Google Scholar -
Kulvinder Kochar Kaur, Allahbadia GN, Singh M. Significance of Fertility Preservation in Patients Undergoing Cancer Chemotherapy Specifically in Adolescents/Young Adults Requiring Alkylating Agent - A Short Communication
View at Publisher | View at Google Scholar -
Kulvinder Kochar Kaur, Allahbadia GN, Singh M. The Mechanism by Which Chemotherapy with use of Alkylating Agents Cause Follicular Activation:Is there any Further Mode for the Loss of the Primordial Follicles? A Short Communication. J Gynecol 2021, 6(3): 000222. DOI: 10.23880/oajg-16000222.
View at Publisher | View at Google Scholar -
ChoyJT, BranniganRE. The determination of reproductive safety in men during and after cancer treatment. Fertil Steril_ 2013;100:1187–91.
View at Publisher | View at Google Scholar -
Meistrich ML. Male gonadal toxicity. Pediatr Blood Cancer 2009;53:261–6.
View at Publisher | View at Google Scholar -
Russell JA, Powles RL, Oliver RT. Conception and congenital abnormalities after chemotherapy of acute myelogenous leukaemia in two men. Br Med J 1976;1:1508.
View at Publisher | View at Google Scholar -
Meistrich ML.“ The effects of chemotherapy and radiotherapy on spermatogenesis in humans . Fertil Steril_ 2013;100(5): doi:10.1016/j.fertnstert.2013.08.010
View at Publisher | View at Google Scholar







