
Case Report | DOI: https://doi.org/BRCA-CR-25-015.
Diagnostic Dilemma of Appendiculo-Ileal Knotting in A 15-Year-Old Female Patient; A Case Report
Abstract
Introduction: Appendicitis and small bowel obstruction are well known surgical emergency cases which usually require emergency admission. Small bowel obstruction can be caused by variety of causes but obstruction caused by appendico-ileal knotting is quite rare. However, even if it is rare and preoperative diagnosis is challenging, it is better to consider in patients who presented with symptoms of appendicitis first or overlap with symptoms of obstruction.
Case presentation: A 15 years old female patient presented to emergency department after a delay at a local health for 06 days with history of crampy abdominal pain and frequent bilious vomiting of 07 days duration which worsen in the last 03 days associated with abdominal distention and high grade fever. On examination she was in shock with cold extremity and in respiratory distress with grossly distended abdomen having diffuse tenderness, guarding and rigidity. Isotonic fluid resuscitation with vasopressor intiated and put on face mask oxygen support as pre-operative resuscitation. Exploratory laparotomy done after resuscitation - About 3.5 litters thin pus mixed with fecal matter, appendicular knot with distal ileum which is frankly gangrenous and perforated. About 20 cm gangrenous distal ileum resected, appendectomy done and distal segment exteriorized as end ileostomy. After thorough peritoneal lavage with warm saline abdominal wall closed with retention suture and patient transferred to surgical ICU. Post-operatively she was kept for seven and half hours as she was on mechanical ventilator, dual vasopressor and other supportive measures but despite this she died of multi-organ failure secondary to refractory septic shock.
Conclusion:
Even though appendiculo-ileal knotting causing small bowel obstruction is rare form of surgical diagnosis, it will cause complicated post-operative period and even death when patients present late. There should be high index of suspicion on appendiculo-ileal knotting as a cause of SBO to peak patients before they decompensate
Introduction
Acute appendicitis is one of the most common surgical emergency case, especially at early ages, who presented with classic appendicitis signs and symptoms or with some complications. Small bowel obstruction(SBO) is a common case of surgical emergency and patients presented with abdominal pain, distension and frequent bilious vomiting. SBO can be caused by post-op adhesion, neoplasms, volvulus, intussuception, hernia, Crohn’s disease, and so on.
Even though SBO is a common surgical emergency, SBO caused by appendicular knotting- an inflamed appendix forming a knot around a small bowel—is very rare and usually an intraoperative diagnosis. Appendicular knotting is one of the rare complications of appendicitis. There are few case reports on appenedicial knotting causing small bowel obstruction, specifically, and there are much fewer reports in pediatric age groups.
Here we report a case of a 15-year-old female patient who presented with symptoms and signs of small bowel obstruction, and she was late at local health center for gastroenteritis treatment and intra-operatively found to have appendiculo-ileal knotting. She was managed with fluid and electrolyte resuscitation, operated and admitted to the surgical intensive care unit but she expired on the day of operation.
Case presentation
A 15-year-old female patient presented to the emergency department with worsening abdominal pain and associated abdominal distension, frequent bilious vomiting and high-grade fever of 04 days duration.
Seven days prior to her emergency arrival she was having nausea, anorexia, a low-grade fever, and abdominal pain that started periumblical and later shifted to the right lower abdomen. She visited a local health center, where she was diagnosed with acute gastroenteritis for which she was given ciprofloxacin with anti-acids as an outpatient and she had improvement from her abdominal pain and fever for 03 days. Starting from the fourth day of her complaint, there was a worsening of crampy abdominal pain, frequent bilious vomiting, abdominal distension and a high-grade fever. She did not have any history of previous surgery, tuberculosis treatment, or any abdominal trauma.
Clinical examination: She was acutely sick, in respiratory distress, and profusely diaphoretic. Her vital signs were blood pressure of 75/50 mmHg, pulse rate of 128–134 beats per minute and feable, respiratory rate of 34–40 breaths per minute, temperature of 38.1 °C, oxygen saturation of 85-88% at room air, and 95% with face mask of 08 litters oxygen support. She had dry buccal mucosa. she uses accessory muscles to breath and she has grossly distended abdomen, guarding, rigidity and diifuse tenderness all over the abdomen, positive sign of fluid collection, hypoactive bowel sound with no visible bowel loops. Digital rectal examination shows stool on examining finger, no mass. Bilateral grade 2 pitting edema, and she was lethargic.
On investigation, blood laboratory result shows
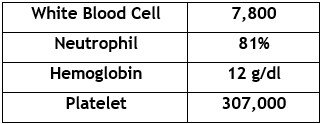
With a working diagnosis of septic shock of Gastrointestinal focus (Generalized peritonitis secondary to gangrenous small bowel to rule out perforated appendicitis), she was on 8 litters of oxygen support with face mask and bilateral IV line secured. She was given 1 unit of normal saline bolus, then put on noradrenaline drip and isotonic fluid resuscitation continued and her blood pressure was maintained in the range of 90/55-95/65. She started ceftriaxone and metronidazole. Nasogastric tube was inserted, and 600 ml of bilious content fluid was coming out. She was also catheterized with no urine output. After mean arterial pressure was maintained within the range of 65–70 mmHg, informed written consent was taken for exploratory laparotomy.
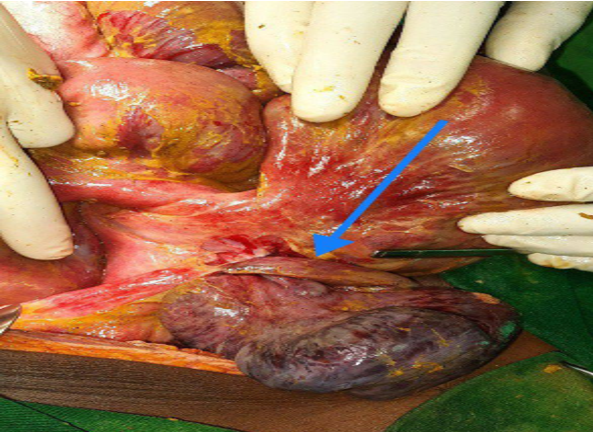
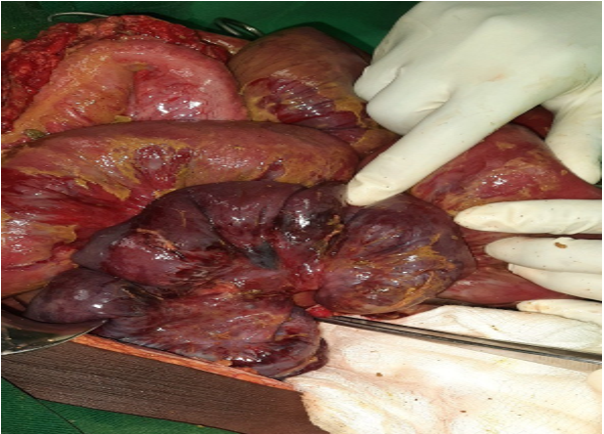
Midline laparotomy done and there was about 3.5 litters of thin pus mixed with fecal matter all over the peritoneum; 20 cm frankly gangrenous distal ileum entangled with the appendix upto the ileocecal valve; there was a 2 cm x 2 cm perforation with spillage of small bowel content at the proximal end of the gangrenous part of the ileum on the anti-mesenteric side; the proximal small bowel was edematous and dilated; the appendicial base looks normal but the tip is involved in the inflammatory process. Other intra-abdominal viscera grossly look normal. Thin pus with small bowel content sucked out, gangrenous part of the small bowel resected and appendectomy done, Peritoneal lavage done thoroughly with warm saline and proximal stump of the ileum exteriorized as end ileostomy, and distal stump closed. The abdomen closed in mass. During the operation, her vital signs were: blood pressure of 90/55–90/60 mmHg on noradrenaline drops of 0.2 micrograms per minute, pulse rate of 124–132 beats per minute, temperature of 37.6-37.9 °C, urine output of 0.3 ml/kg/hr, and she was transferred to the surgical ICU, where she was on a mechanical ventilator, noradrenaline drops of 0.2 ug/kg/min, IV antibiotics continued, Cimetidine 200 mg IV BID was added, and she was on continuous ICU monitoring.
But starting 3 hours post-operatively, her blood pressure dropped to a level of 75/55 mmHg, and her oxygen saturation was 89–91%. For this, hydrocortisone 100 mg IV given and dopamine 5 ug/kg/min added, and her blood pressure maintained within the range of 90/60–95/60 for 4 hours. However, at the 7th post-operative hour, her blood pressure became unrecordable despite the fact that the dual vasopressor was escalated, and she died at the 7th and a half post-operative hour with refractory septic shock.

Discussion
Small bowel obstruction is one of the major causes that need surgical emergency admission and is a leading cause of morbidity and financial expenditure across the world. Adhesion is still one of the leading causes of small bowel obstruction in western society [1]. But when we come to our country, Ethiopia, among the common leading causes of small bowel obstruction, small bowel volvulus is by far the most common followed by intussusception and adhesion, respectively. The least common causes of small bowel obstruction are hernia and other intestinal knotting cases; in intestinal knotting cases, appendiculo-ileal knotting is a rare form of knotting [2] .
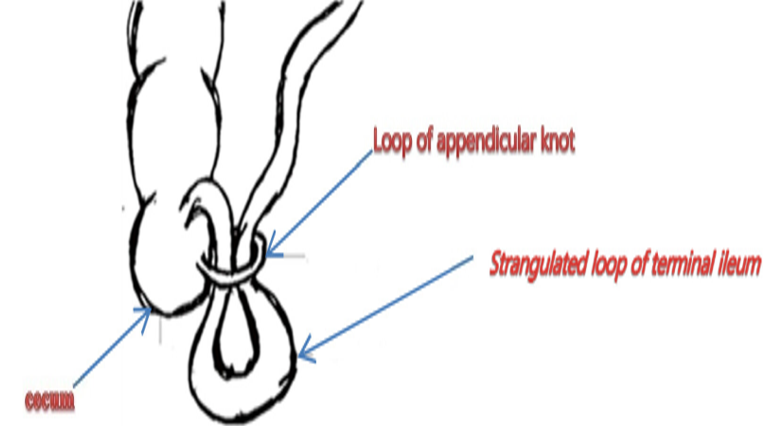
An appendicular knot is a mechanical obstruction with the form of a knot or a ring-like entrapment of the segmental part of the ileum by the appendix, which will form a closed loop obstruction and lately end up with bowel ischemia and strangulation. It has different names by different authors, like appendicular band syndrome and appendicular tie syndrome, but by all means, the appendix causing SBO by forming a knot is extremely rare [4]. The possibility of diagnosing appendicular knotting preoperatively is quite difficult and challenging since patients are not usually present with a clinical presentation of appendicitis. An appendicular knot forming SBO is a form of intraoperative diagnosis after patients present with signs and symptoms of SBO[5]. Though diagnosing appendicular knot as an etiology of SBO preoperatively, suspecting the possibility is better when the patient presents with symptoms of SBO after manifesting signs and symptoms of appendicitis for certain periods of time. The preoperative investigations depend on the patient's clinical condition. When the patient's hemodynamic status is stable, they can be investigated with a plain abdominal x-ray or computed tomography with other basic blood investigations, but even though abdominal computed tomography is diagnostic for acute appendicitis, the case of the appendix causing SBO is questionable [6, 7]. The other option of approach for an uncertain pre-operative diagnosis and a patient with a normal range of vital signs is diagnostic laparoscopy [8, 9]. Case-based suspicion and curiosity to prevent bowel ischemia and gangrene or sepsis are essential for diagnosing them early and giving emergency surgical intervention [10].
Our patient was one of the delayed presenters; she came to our emergency department after seven days of delay. While she arrived, her hemodynamic state was unstable, and despite our emergency resuscitation and surgical intervention, she died of refractory septic shock.
After exploratory laparotomy, there will be two options for bowel management. The first is just appendicular band release, and doing an appendectomy will be enough during a viable entrapped ileum. The second option is appendicular band release, appendectomy with ileal resection and anastomosis, or ileostomy, depending on the viability of the bowel [10].
Delayed presentation or missdiagnosis of patients with a lack of clarity for early diagnosis of appendiculo-ileal knotting will cause bowel strangulation and sepsis, which leads to a complicated post-operative period and death [5, 11].
Conclusion
Even though appendiculo-ileal knotting causes small bowel obstruction and is a rare form of surgical diagnosis, early investigation and surgical management are necessary. When patients are delayed for emergency presentation, it will cause a complicated post-operative period and even lead to death after they decompensate.
Declarations
Ethical clearance
The case report has been submitted to the School of Medicine at the University of Gondar, Ethiopia, for ethical board review and approval as an ethically sound report.
Consent
Written informed consent was taken from the parents for publication of case report and any accompanying image. A copy of written consent is available for review for the editor in chief of this journal
Availability of data and materials
The author of this manuscript is willing to provide any additional information regarding the case report.
Conflict of interest
There were no disclosed potential conflicts of interest related to this article.
Authors contribution
The case report was conceptualized, written, and edited by all authors. It is agreed that each and every author will take full responsibility.
Funding
All authors declare that no financial support was received from any organization for the submitted report
References
-
Molla, Y.D., et al., Ileo-ileal knot causing acute gangrenous small bowel obstruction: a case report. Journal of Medical Case Reports, 2024. 18(1): p. 72.
View at Publisher | View at Google Scholar -
Fekadu, G., et al., Epidemiology and causes of intestinal obstruction in Ethiopia: A systematic review. SAGE Open Medicine, 2022. 10: p. 20503121221083207.
View at Publisher | View at Google Scholar -
Abule, T., T. Chebo, and B.B. Billoro, Appendico‐ileal knotting causing small bowel obstruction: A case report. Clinical Case Reports, 2022. 10(5): p. e05878.
View at Publisher | View at Google Scholar -
Ranjan, A., K. Kumari, and S. Jha, Acute small bowel obstruction as a result of an appendicular knot encircling the terminal ileum: an exceptionally rare case report. Int J Med Sci Public Health, 2015. 4: p. 426-429.
View at Publisher | View at Google Scholar -
Wondwosen, M., T. Tantu, and D. Zewdu, Appendiceal knotting causing small bowel obstruction: A rare case report. International Journal of Surgery Case Reports, 2022. 93: p. 106970.
View at Publisher | View at Google Scholar -
IDOWU, N.A., et al., Appendico-Ileal Knotting: A Rare Cause of Strangulated Small Bowel Obstruction. Ethiopian Journal of Health Sciences, 2024. 34(2).
View at Publisher | View at Google Scholar -
O’Donnell, M., et al., Small bowel obstruction secondary to an appendiceal tourniquet. Irish journal of medical science, 2009. 178: p. 101-105.
View at Publisher | View at Google Scholar -
Thanapal, M., Z. Ariffin, and M. Azizi, Rare complication of appendix: small bowel gangrene caused by the appendicular knot. Med J Malaysia, 2017. 72(6): p. 370-1.
View at Publisher | View at Google Scholar -
Bhandari, L. and P. Mohandas, Appendicitis as a cause of intestinal strangulation: a case report and review. World journal of emergency surgery, 2009. 4: p. 1-4.
View at Publisher | View at Google Scholar -
Chatterjee, C., et al., Appendiceal knotting causing small bowel strangulation. Journal of Research in Medical Sciences: the Official Journal of Isfahan University of Medical Sciences, 2014. 19(10): p. 1016.
View at Publisher | View at Google Scholar -
Rodriguez Zorro, A. and J.H. Vivas Diaz, Death caused by appendicular knotting and small-bowel strangulation in a child: a case report and review. Medicine, Science and the Law, 2018. 58(2): p. 115-118.
View at Publisher | View at Google Scholar







