
Review Article | DOI: https://doi.org/BRCA-RW-25-013
Aspergillus Infections: Prevention, Laboratory Diagnosis, and Pathophysiology
Abstract
Aspergillus spp., are hyaline molds causing allergic, invasive and toxin mediated infections and other disorders. They are also important causes of mycetoma-like lesions. Diagnosis of infections caused by Aspergillus spp. involve culture, biopsy and microscopy. Treatment consists of triazoles. Prevention is the key. All these aspects have been reviewed here.
Introduction:
Aspergillus infections, caused by the filamentous fungi of the Aspergillus species, are a significant concern in both immunocompromised and immunocompetent individuals. Neutropenic individuals are at risk of invasive Aspergillosis.These infections can range from harmless colonization to severe allergic or invasive diseases, depending on the host’s immune status.
Pathophysiology
Aspergillus species are ubiquitous in the environment, particularly in soil. The infection begins when aerosolized conidia (spores) are inhaled. In immunocompromised individuals, such as those undergoing stem cell transplantation or receiving immunosuppressive therapy, the spores can germinate and develop into hyphae, which invade blood vessels and cause hemorrhagic necrosis and infarction. In immunocompetent individuals, chronic pulmonary aspergillosis (CPA) can occur, often in those with underlying lung conditions1.Sometimes they colonize the lung cavities produced by pulmonary TB, caused by Mycobacterium tuberculosis.
The angioinvasive nature of the fungus makes predisposed individuals prone to suffer from invasive aspergillosis (IA). Neutropenia also favours this condition.
Clinical Spectrum
The clinical spectrum of aspergillosis varies widely:
Infections caused by A. fumigatus and A. flavus:-
a.Invasive Aspergillosis (IA): Mostly affects immunocompromised patients and presents with non-specific symptoms such as fever, cough, and pleuritic pain. Early diagnosis is crucial for improving prognosis1. The small size of A. fumigatus makes it highly suitable for causing invasive infections.
b.Chronic Pulmonary Aspergillosis (CPA): Affects individuals with underlying lung conditions and can lead to the formation of aspergillomas (fungal balls) in lung cavities1. This is seen more comnly after cavity caused by pulmonary Tuberculosis.
c.Allergic Bronchopulmonary Aspergillosis (ABPA): An allergic reaction to Aspergillus species, often seen in patients with asthma or cystic fibrosis1. It can cause restrictive chest disorder. There is expulsion or expectoration of mucus plugs or yellow-brown fungal “plugs”. Chest X ray may be diagnostic. It is most commonly caused by A. fumigatus and rarely by A. flavus.
d. Invasive and allergic rhinosinusitis or Allergic fungal rhinosinusitis (AFRS).
Infections caused by A. niger:-
The huge size of spores of A. niger makes it unfit for causing invasive infections. However, it may cause otitis externa especially after ear trauma.
Infections caused by A. nidulans:_
Mycetoma like lesions are produced by A. nidulans.
Mycotoxins
Aflatoxin is produced by toxigenic strains of A. flavus and A. parasiticus 2. These toxins are found mostly in grains like rice and peas, stored in cold, humid places for a liong time. Long term consumption may cause hepatitis and eventually liver fibrosis or cirrohosis and hepatocellular carcinoma. Aflatoxins are of 3 types:- B1, B2, G1, G2 , M1 and M2. Aflatoxin B1 gives blue fluorescence under UV light while aflatoxin G1 yields green fluorescence. are M1 and M2 toxins are the hydroxylated metabolites of AFB1 and AFB23.
Medicinal uses of Aspergillus spp.:--
A. terreus can act as source of specific drugs called statins ( which are given to lower cholesterol levels in man). The statins are a group of drugs which inhibit HMG-CoA reductase and help lower cholesterol production. The statins were initially discovered in fungi and for many years fungi were considered the only source for statins4.
Laboratory diagnosis: Culture, biopsy and immunodiffusion tests are mainstay for diagnosis.
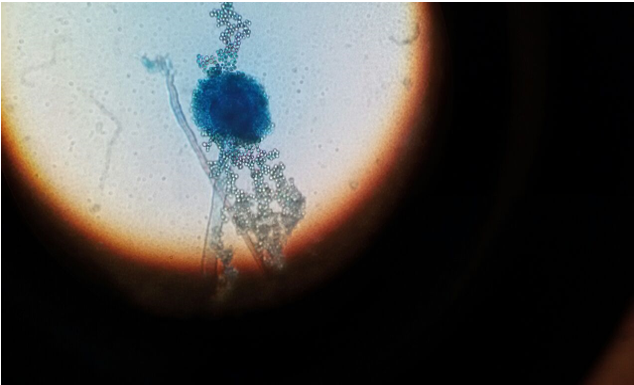
Sputum or BAL are ideal samples for diagnosis invasive pulmonary aspergillosis. In these cases, microscopy with 10% KOH mount and culture will clinch the diagnosis, substantiated by demonstration of hyphae with acute angled branching on Histopathology. Microsocpy from culture shows stipe over hyphae, and metulae or phialdies on top of stipe, with rows of conidia on top of the phialides. If philaides are see in 1 row only, it is called uniseriate fungus, while if 2 rows are present, it is called biseriate fungus. A. flavus is commonly biseriate while A. fumigatus is uniseriate.
In culture one should always observe the straight(obverse) as well as reverse side of the colonies. In Aspergillus spp. the reverse aspect is always white or colourless, while obverse side is yellow-green in A. flavus, black later after initial whote growth in A. niger and mousy-grey in case of A. fumigatus. In A. nidulans and A. versicolor, shades of yellow, brown and grey are noticeable in obverse aspect, while A. terreus yields tan-to brown colonies. In A. nidulans, the head or vesicle is hemispherical while Hulle cells are abundant. Colour of mycelium is due to the colour of conidia, e.g. in A, noiger the colour of conidia is black. For confirming Aspergillus spp., one should go for microscopic observation of Lactophenol cotton blue mount, showing typical microscopic morphology. For showing typical colonies and spores, culture on Czapek-Dox agar is recommended. Slide culture on Potato dextrose agar also induces typical conidiation and aids in diagnosis.
Differential microscopic morphology of some important Aspergillus spp. with respect to vesicle(head) and phialides/metulae is shown in table 1 below:_-
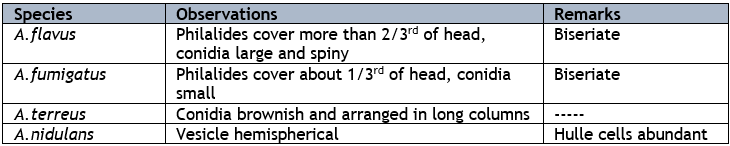
It has to be remembered that A. fumigatus can grow at 45 °C , or is thermotolerant. Others are not thermotolerant.
Accurate and timely diagnosis of aspergillosis is essential for effective management. Other diagnostic methods include:-
a.Radiology: High-resolution CT scans of the chest, sinuses, and brain are useful for detecting invasive aspergillosis, including invasive Aspergillus sinusitis1.Chest X ray bshows typical “tram-track” or “finger in glove” appearance in ABPA cases.
b. Non-culture-based methods like AsperGenius®, MycAssay Aspergillus®, and MycoGENIE® are also used now5. The AsperGenius test can be done directly from clinical specimens.
Serological Tests: Serum Aspergillus galactomannan antigen test is a valuable tool for early diagnosis1. PLATELIA ELISA can also be done to detect galactomannan antigen6. It is a commercially available sandwich ELISA which detects galactomannan by means of a rat monoclonal antibody (EB-A2), which is used as both detector and captor. Gel diffusion test is useful for screening AFRS and ABPA with precipitins detected against Aspergilluis spp. This test is done in small petri dishes incubated at room temperature.

Prevention
Preventing aspergillosis involves reducing exposure to Aspergillus spores, particularly in high-risk individuals. There are a number of preventive measures that can be carried out in the case of Aspergillus niger infections especially for the immunocompromised. Key preventive measures include:
- Dust Exposure: It is advisable to keep off places that generate excessive levels of dust, such as, construction sites or areas under excavation. Where it is unavoidable, consider wearing an N95 respirator to limit exposure5.
- One can wear face masks where there is a high chance of finding Aspergillus spores, like in construction sites.
- Maintain Hygiene: It is essential to have clean environments by disinfecting surfaces. This ensures the level of contamination by fungal spores is lower7.
- Wear Protective Clothing: Clothes such as long sleeves, pants and gloves are recommended for use during soil or dust related activities such as gardening6.
- Skin Injury: Activities that promote excessive soil or dust exposure should be curtailed. If a skin injury occurs, it should be well cleaned with soap and water in order to prevent disease².
- Long-term Antifungal Therapy: Providers of healthcare have also recommended having long term antifungal therapy for targets who are very susceptible, these include patients with history of stem cell transplants or organ transplants6.
- Moisture and Mold Exposure: It is important to ensure that there is adequate ventilation within your residence as this limits growth of mold and moisture7.
- Routine Check-ups: People who are at constant risk of developing these infections need to get constant professional attention and blood tests may be necessary for these people.
- Environmental Control: Minimizing exposure to dust and soil, especially in hospital settings. Air can be surveyed by settle plate method (using SDA plate) to look out for spores of A. flavus.
- Prophylactic Antifungal Therapy: For high-risk patients, such as those undergoing stem cell transplantation1.
Management
The management of aspergillosis depends on the type and severity of the infection.
Invasive Aspergillosis: Antifungal agents such as isavuconazole and voriconazole are the treatments of choice. In fact, the USDFA has approved Isavuconazole as primary therapy for Invasive Aspergillosis (IA)7. Lipid-based formulations of amphotericin B are potent alternatives.
Chronic Pulmonary Aspergillosis: Treatment varies , depending on the type and severity of the infection. Surgical options need to be considered in cases of complicated sinusitis involving eye or optic nerve, and brain abscess following cavernous sinus thrombosis, or aspergilloma causing bleeding into the lungs8.
Allergic Bronchopulmonary Aspergillosis: Management includes corticosteroids and antifungal therapy.
Discussion
Aspergillus spp. are ubiquitous in the environment. They are important causes of many superficial, allergic and deep-seated infections. Proper suspicion and management is essential to address these infections.
Conclusion
Aspergillus infections pose a significant threat, particularly to immunocompromised individuals. Early diagnosis and appropriate management are crucial for improving patient outcomes. Continued research and advancements in diagnostic methods and antifungal therapies are essential for combating these infections effectively.
References
-
Chronic pulmonary aspergillosis. https://www.sciencedirect.com/topics/agricultural-and-biological-sciences/chronic-pulmonaryaspergillosis#:~:text=Chronic%20Pulmonary%20Aspergillosis%20(CPA)&text=The%20most%20frequent%20underlying%20diseases,common%20conditions%20worldwide%2C%20and%20sarcoidosis.last accessed 06.11.24.
View at Publisher | View at Google Scholar -
Dhakal A, Hashmi MF, Sbar E. Aflatoxin Toxicity. [Updated 2023 Feb 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557781/ last accessed 07.11.24.
View at Publisher | View at Google Scholar -
Pradeep ML, Mahato DK. , Madhu K , Mohanta TK. , Kang SG. Aflatoxins: A Global Concern for Food Safety, Human Health and Their Management. Frontiers Microbiol 2017;7
View at Publisher | View at Google Scholar -
https://www.frontiersin.org/journals/microbiology/articles/10.3389/fmicb.2016.02170
View at Publisher | View at Google Scholar -
Subhan M, Faryal R, Macreadie I. Exploitation of Aspergillus terreus for the Production of Natural Statins. J Fungi (Basel). 2016 Apr 30;2(2):13. doi: 10.3390/jof2020013.
View at Publisher | View at Google Scholar -
White PL, Posso RB, Barnes RA. Analytical and Clinical Evaluation of the PathoNostics AsperGenius Assay for Detection of Invasive Aspergillosis and Resistance to Azole Antifungal Drugs Directly from Plasma Samples. J Clin Microbiol. 2017 Aug;55(8):2356-2366. doi: 10.1128/JCM.00411-17.
View at Publisher | View at Google Scholar -
Klont RR, Mennink-Kersten MASH, Verweij PE. Utility of Aspergillus Antigen Detection in Specimens Other than Serum Specimens, Clinical Infectious Diseases, 2004;39(10):1467–1474. https://doi.org/10.1086/425317.
View at Publisher | View at Google Scholar -
Batista MV, Ussetti MP, Jiang Y, Neofytos D, Cortez AC, Feriani D, Schmidt-Filho J, França-Silva ILA, Raad I, Hachem R. Comparing the Real-World Use of Isavuconazole to Other Anti-Fungal Therapy for Invasive Fungal Infections in Patients with and without Underlying Disparities: A Multi-Center Retrospective Study. J Fungi (Basel). 2023 Jan 27;9(2):166. doi: 10.3390/jof9020166.
View at Publisher | View at Google Scholar -
Aspergillosis. https://www.mayoclinic.org/diseases-conditions/aspergillosis/diagnosis-treatment/drc-20369623. Last accessed 06.11.24.
View at Publisher | View at Google Scholar








