
Research Article | DOI: https://doi.org/CCSRR-RA-24-012
Morphological And Morphometric Analysis of The Triangle of Auscultation in Human Fetuses: An Approach to Thoracic Surgery finance
Abstract
Introduction
The triangle of auscultation (TA) is an area on the back delimited by the scapula, trapezius muscle, and latissimus dorsi muscle. Due to its thinner thickness, it facilitates pulmonary auscultation and surgical procedures, reducing complications and pain. The blood and nerve supply to the TA is provided by the thoracodorsal, superficial cervical, and dorsal scapular arteries, and by the thoracodorsal, accessory, and spinal nerves C3 to C4. This study aims to perform a morphological and morphometric analysis of the triangle of auscultation.
Materials and Methods
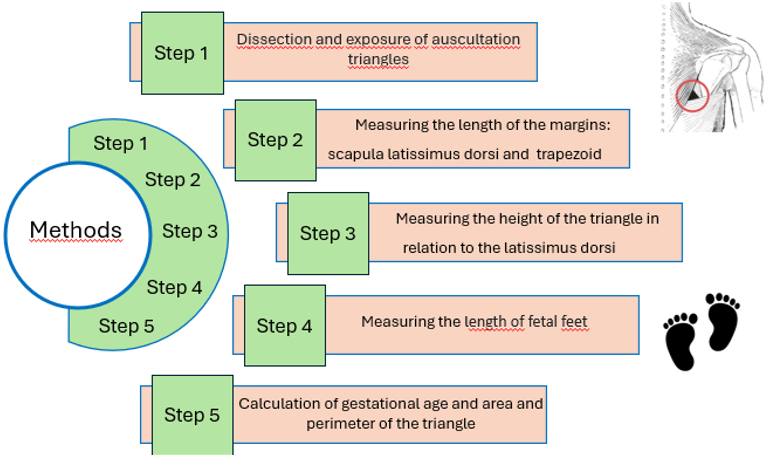
The sample included 40 fetuses (20 male and 20 female), totaling 80 TAs. To determine the gestational age of the fetus, the hallux-calcaneal length measurement was used. In the morphological analysis, the TAs were classified as acute-angled, right-angled, or obtuse-angled based on the margins and internal angles. For the morphometric analysis, a caliper was used to measure the length of the margins of the scapula, latissimus dorsi, and trapezius. Statistical analysis was performed based on the generalized linear model and the G test.
Results
It was found that the mean gestational ages of the female and male fetuses were 28.94 (3.23) and 28.38 (3.82) weeks, respectively. Homogeneity of the measurements of the area, perimeters, and margins of the TA was demonstrated in relation to both the side of the triangle and the sex of the fetus. Gestational age stood out as a variable with significant influence on the characteristics of the triangle.
Conclusion
Through the morphological and morphometric analysis of the TA, it was demonstrated that variables such as sex, side, and morphology do not have significant influence, but age stood out as a factor influencing the margins, perimeter, and area.
Introduction
The pulmonary auscultation triangle (TA) is a clinically valuable region located dorsally on each side of the trunk. The area is bounded: medially by the lateral border of the lower part of the trapezius; laterally by the vertebral border of the scapula; and inferiorly by the superior margin of the latissimus dorsi muscle [1]. Deeply, forming the floor of the triangle are the rhomboid major, iliocostal muscles, and fascial lamina. These two muscles form the first layer of tissue towards the interior of the thoracic cavity. Forming a second layer are the 7th intercostal space and the 6th and 7th ribs [2].
Due to its thinner thickness, the TA offers low resistance for thoracic sound auscultation and mechanical resistance to surgical procedures, making it useful for a wide range of invasive approaches to the thorax [3]. Access to internal thoracic structures through thoracotomy or thoracoscopic surgery, pleurectomy, lobectomy, tumor excision in the ventral scapular region, and nerve blocks are some of the surgical procedures that result in lower risks of complications and are less painful for the patient when performed through this triangle [4-8] . In addition, it can provide a shorter postoperative period and a faster recovery.
The blood and nerve supply of the triangle are the same as those structures that anatomically form it. The thoracodorsal artery is responsible for vascularizing the latissimus dorsi muscle, and the superficial cervical artery and the dorsal scapular artery are responsible for the trapezius and rhomboid major muscles, respectively [1]. Regarding nerve supply, the thoracodorsal nerve, accessory nerve, and spinal nerves C3 to C4, as well as the dorsal scapular nerve, are responsible for the innervation of the latissimus dorsi, trapezius, and rhomboid major muscles [1].
Knowledge of thoracic anatomical regions is important for clinical assessment, diagnosis, and therapeutic success. Despite the knowledge about the area of the auscultation triangle, its morphometric evaluation has not been properly characterized. The objective of this study was to conduct a morphological and morphometric analysis of the pulmonary auscultation triangle.
Materials And Methods
Materials And Methods
Forty human fetuses belonging to the Laboratory of Human Anatomy of the Federal University of Sergipe in Sergipe, Brazil were used. The fetuses were obtained according to Law 8.501 of 1992, which deals with the use of unclaimed cadavers for studies and research. Fetuses of both sexes (20 male and 20 female) were included, which were fixed in formalin, and showed no evidence of gross abnormalities of the chest. The gestational age of fetuses was obtained from the equation GA=8.2982 + (0.38764 F), in which GA is the gestational age and F is the measure of the length of the calcaneus-hallux[9] that was measured with a digital caliper of precision of 0.01 mm.
Morphological Analysis
A total of 80 TAs were analyzed. For the morphological analysis, the margin of the scapula, the trapezius muscle, the latissimus dorsi and the internal angles of the TA were observed with the naked eye, to classify them in 3 types:
Type I) Acute-angled: all internal angles less than 90º.
Type II) Obtuse-angled: one of the internal angles greater than 90º.
Type III) Right-angled: one of the internal angles was approximately 90º.
After morphological observation, the fetuses were photographed. Each of them was placed on a smooth and non-reflective surface and, to avoid distortion, it was positioned in the center of the lens with the camera in a position perpendicular to the surface of the TA. Images were obtained using a Nikon 5100 digital camera (Canon Inc., Japan) with a 100mm macro lens.
Morphometric Analysis
Under natural light, using a digital caliper with precision of 0.01 mm, measurements were made of the length of the margins of the scapula, the trapezius, the latissimus dorsi and the height of the TA in relation to the latissimus. The area and perimeter of the TAP were calculated based on taking the following measures:
Area of the TA = (length of the latissimus x height of the TA) / 2
Perimeter of the TA = sum of the lengths of the medial margin of the scapula + trapezius + latissimus dorsi.
All the steps of the methodology are shown in figure 1.
Statistical Analysis
The sample characteristics were utilized through descriptive measures such as minimum and maximum values, median, quartiles, mean, and standard deviation. The generalized linear model was used for the treatment of non-parametric and multivariable sampling, which allowed the association between a dependent variable and independent variables. Thus, a bilateral analysis of the area, perimeter, and length of the TA margins was performed based on the sex and age of the fetus. To evaluate whether there was a difference between the quantity of triangle types between the right and left sides, as well as between male and female sexes, the G Test was used. Simple linear regression was used to explain the relationship between the respective margins of the triangle on each side. The analyses were carried out using the BioEstat 5.3 software.
Results
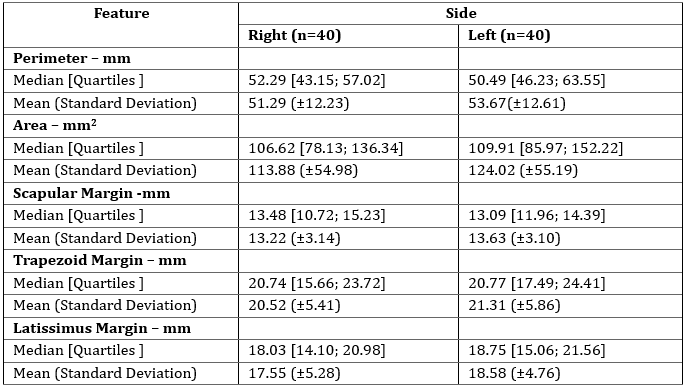
Eighty TA from forty human fetuses were analyzed, twenty males and twenty females. The mean and median gestational ages of the fetuses were 28.66 (3.51) and 28.16 [25.97; 31.02] weeks, respectively. In the analysis of the TA data, a similar measurement of the area, perimeters, and lengths of the TA margins was observed between the sides (Table 1).
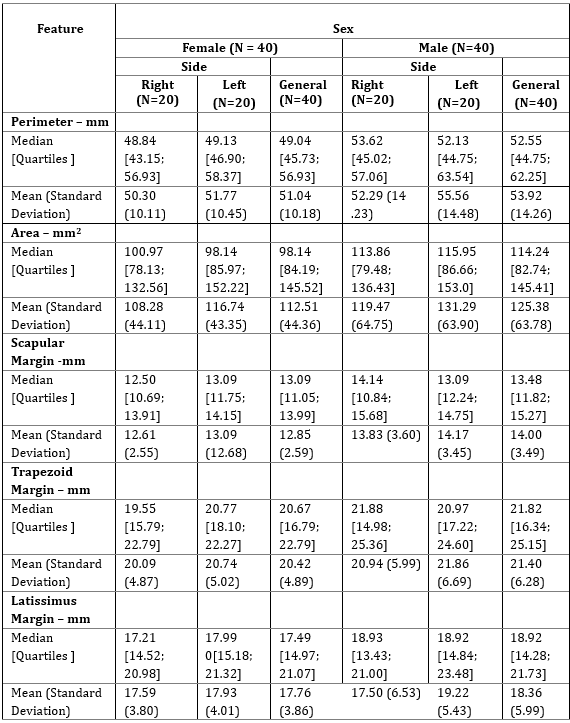
In the analysis of gestational age according to sex, it was found that the mean gestational ages of female and male fetuses were 28.94 (3.23) and 28.38 (3.82) weeks, respectively. A slightly larger perimeter, area, and lengths of the TA margins were found in male fetuses; however, these were insufficient to demonstrate heterogeneity (Table 2).
Fetal gestational age had a significant influence on the perimeter (p = 0.0004), area (p = 0.0001), and lengths of the trapezius margin (p = 0.0003), latissimus dorsi (p = 0.0074), and scapula (p = 0.0035), indicating an increase in these measurements with age (Figure 2).
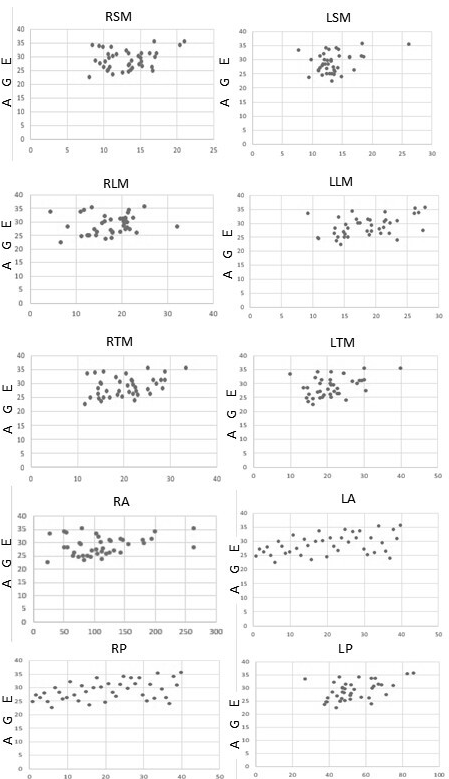
RSM - Right Scapular Margin
LSM - Left Scapular Margin
RLM - Right Latissimus Margin
LLM - Left Latissimus Margin
RTM - Right Trapezius Margin
LTM - Left Trapezius Margin
RA - Right Area
LA - Left Area
RP - Right Perimeter
LP - Left Perimeter
On the other hand, variables such as side and sex did not have a significant impact on the TA measurements.
Regarding the morphology of the triangle of auscultation, there was homogeneity in the types of triangles observed, on the right and left sides (p = 0.1506), as well as between sexes (p = 0.1244). On the right side, 35.0% of the triangles were acute-angled, 20.0% obtuse-angled, and 45.0% right-angled. On the left side, 52.5% were acute-angled, 22.5% obtuse-angled, and 25.0% right-angled (Figure 3).
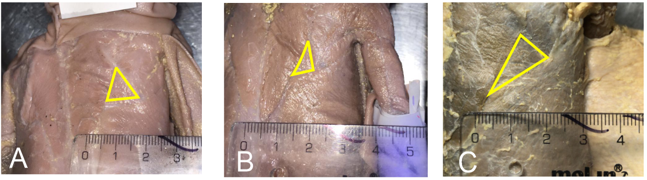
- Acute-angled
- Right-angled
- Obtuse-angled
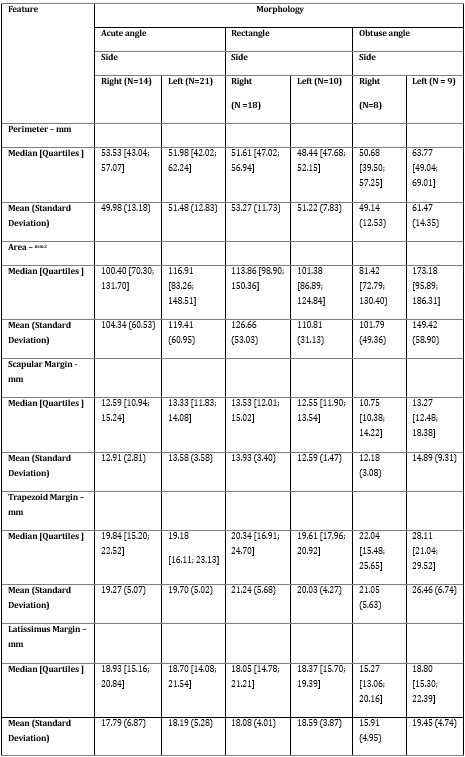
The morphometric analysis based on the types of triangles can be seen in Table 3.
Discussion
The pulmonary auscultation triangle (TA) is an anatomical region present dorsally on each side of the trunk, characterized by having a thinner muscle mass, thus facilitating pulmonary auscultation. For this purpose, the patient should be instructed to cross their arms over their chest and lean forward. Additionally, this area of pulmonary auscultation serves as a field for surgical procedures, ensuring easy access and good patient recovery.
Among these procedures, thoracotomy stands out: a surgical procedure to open the chest that allows access to internal structures such as the lungs, heart, and vascular structures[1]. In this context, Buratto and Konstantinov [10] mentioned that thoracotomy performed in children with aortic coarctation is usually done via a posterolateral approach, involving the incision of the latissimus dorsi and serratus anterior muscles, while the approach through the auscultation triangle ensures that these muscles are spared, without compromising the repair of the coarctation.
Khan et al., [11] compared thoracotomy via the triangle of auscultation with posterolateral thoracotomy, highlighting the difference between the incision and preservation of the latissimus dorsi muscle. These authors noted that patients undergoing the procedure via this triangle had greater preservation of shoulder adduction, a movement in which the latissimus dorsi muscle is the major contributor.
Caronia et al., [12] compared uniportal video-assisted lobectomy performed via anterior, posterior through the auscultation triangle, and posterior via the posterior axillary line. It has been discussed that access via the axillary line would enable better visualization of the pulmonary hilum compared to the anterior incision video-assisted surgery technique. Additionally, the procedure via the triangle would enable a quick transition to video-assisted thoracotomy for surgeons unfamiliar with this access but who use the traditional posterolateral approach.
Diaz and Azar [13] discussed the use of the TA in video-assisted chest wall stabilization surgeries, highlighting the non-division of muscles and lower morbidity. In procedures performed on cadavers, they pointed out that in cases of lateral and posterolateral rib fractures, the triangle of auscultation would facilitate the surgery.
Other studies have sought more possibilities for procedures performed through the triangle of auscultation, such as in cases of esophageal atresia, lobectomy, and pleurectomy[4,7,14]. Thus, the variety of procedures that the triangle enables is highlighted, as well as benefits such as a shorter postoperative recovery period.
The trapezius margin was the longest, followed by the latissimus dorsi margin, and lastly, the scapular margin. Additionally, the average area of the triangles was homogeneous regardless of the morphological types. The statistical analysis showed no significant differences regarding the sides of the triangles, morphology, or the sex of the fetus. However, it highlighted the influence of age on the development of the triangle, as the three margins of the triangle, the area, and perimeter increased with gestational age. From a clinical perspective, there would be no difference in interventions made through the triangle between men and women, or on the right or left side. However, access to the thoracic region would be facilitated according to the individual's age, considering the larger area of the triangle. It is also worth noting that patients under one year of age who undergo thoracotomy have a higher risk of subsequent scoliosis due to the probable influence of stress on the ribs and the costovertebral joint[15]. Nevertheless, there are reports of procedures performed on children through the triangle, highlighting greater muscle conservation and better scoliosis outcomes compared to conventional thoracotomies[16].
The described applications indicate that more anatomical studies on the triangle of auscultation are necessary to better explore this anatomical area clinically and surgically.
Conclusion
The TA facilitates access to thoracic structures, enabling invasive procedures and examination through auscultation. In the present study, the morphological and morphometric analysis of the triangle demonstrated that variables such as sex, side, and morphology do not have a significant influence, but age stood out as a factor influencing the margins, perimeter, and area. More anatomical studies and clinical observations need to be conducted to verify how these factors can enhance procedures in patients.
Acknowledgment
The authors wish to sincerely thank those who donated their bodies to science so that anatomical research could be performed. Results from such research can potentially improve patient care and increase mankind's overall knowledge. Therefore, these donors and their families deserve our highest gratitude.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
RESEARCH ETHICS COMMITTEE APPROVAL
The study was approved by the Universidade Federal de Sergipe Research Ethics Committee under hearing number 5.754.214 and CAAE: 64361122.5.0000.5546. The study followed the ethical guidelines established by the Declaration of Helsinki.
Declaration Of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
-
Malik N, Tedder BL, Zemaitis MR. Anatomy, Thorax, Triangle of Auscultation. 2023 Jul 24. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. PMID: 30969656.
View at Publisher | View at Google Scholar -
Leslie Pace, J. Anatomical triangles. Chest-piece. 1966;2(6):43-49. Neck triangles
View at Publisher | View at Google Scholar -
Greiffenstein P, Tran MQ, Campeau L. Three common exposures of the chest wall for rib fixation: anatomical considerations. J Thorac Dis 2019;11:S1034–43.
View at Publisher | View at Google Scholar -
Goh DW, Brereton RJ. Triangle of auscultation thoracotomy for esophageal atresia. Journal of Thoracic and Cardiovascular Surgery 1992;103:14–16.
View at Publisher | View at Google Scholar -
Horowitz MD, Ancalmo N, Ochsner JL. Thoracotomy through the auscultatory triangle. Ann Thorac Surg 1989;47:782–783.
View at Publisher | View at Google Scholar -
Lau OJ, Shawkat S. Pleurectomy through the triangle of auscultation. Thorax. 1982; 37: 945-946.
View at Publisher | View at Google Scholar -
Nazarian J, Down ; G, Lau ; O J. Pleurectomy Through the Triangle of Auscultation for Treatment of Recurrent Pneumothorax in Younger Patients Evaluation of 60 Consecutive Cases. n.d.
View at Publisher | View at Google Scholar -
Stamenovic D, Messerschmidt A. Posterior uniportal video-Assisted thoracoscopic surgery for resection of the apical segment of the right lower lobe followed by completion lobectomy. Interact Cardiovasc Thorac Surg 2017;24:644–645.
View at Publisher | View at Google Scholar -
Goldstein I, Reece EA, Hobbins JC. Sonographic appearance of the fetal heel ossification centers and foot length measurements provide independent markers for gestational age estimation. Am J Obstet Gynecol 1988;159:923–926.
View at Publisher | View at Google Scholar -
Buratto E, Konstantinov IE. Commentary: Muscle-sparing thoracotomy in children: is it safe for coarctation repair? JTCVS Tech 2020;3:257–258.
View at Publisher | View at Google Scholar -
Khan IH, McManus KG, McCraith A, McGuigan JA. Muscle sparing thoracotomy: a biomechanical analysis confirms preservation of muscle strength but no improvement in wound discomfort. Eur J Cardiothorac Surg. 2000 Dec;18(6):656-661
View at Publisher | View at Google Scholar -
Caronia FP, Arrigo E, Fiorelli A. Uniportal video-assisted lobectomy through a posterior approach. J Thorac Dis 2017;9:4057–4063.
View at Publisher | View at Google Scholar -
DIaz JJ, Azar FK. Minimally invasive chest wall stabilization: A novel surgical approach to video-assisted rib plating (VARP). Trauma Surg Acute Care Open 2019;4.
View at Publisher | View at Google Scholar -
Gimferrer JM, Belda J, Catalán M, Serra M, Rubio M, Iglesias M. Lobectomía videoasistida a través del triángulo auscultatorio en el tratamiento quirúrgico del carcinoma broncopulmonar. Experiencia preliminar. Arch Bronconeumol 2003;39:87–90.
View at Publisher | View at Google Scholar -
Roclawski M, Pankowski R, Smoczynski A, Ceynowa M, Kloc W, Wasilewski W, et al. Secondary scoliosis after thoracotomy in patients with aortic coarctation and patent ductus arteriosus. Stud Health Technol Inform 2012;176:43–46.
View at Publisher | View at Google Scholar -
Berset SG, Dave H, Balmer C, Nowacka A, Pfister R, Myers PO, et al. Muscle-sparing aortic coarctation repair. JTCVS Tech 2020;3:249–256.
View at Publisher | View at Google Scholar








